Download
1 / 29
290 likes | 458 Views
Hansen MS, Blair DF, Nelson SM, Farrar EL: Wenatchee High School/BioSports, Wenatchee Washington. Spine Injury in a Competitive Cyclist. Background.

E N D
Hansen MS, Blair DF, Nelson SM, Farrar EL: Wenatchee High School/BioSports, Wenatchee Washington Spine Injury in a Competitive Cyclist
Background • Our subject is a 49 y/o male competitive recreational cyclist (PT/ATC) who crashed on a time trial bike while competing in a multi-event relay on June 29, 2008. • He failed to negotiate a curve and crashed into a rock going approximately 40 miles per hour.
Background (cont.) • At the time of impact, the subject was knocked unconscious and did not regain consciousness for twenty minutes. • The subject had difficulty breathing, chest pain, paresthesia/numbness and motor loss in the left hand/elbow and neck pain.
Differential Diagnosis • cervical/thoracic fractures • spinal cord injury • brachial plexus neuropraxia/neurotemesis • rib fractures • pneumothorax • closed head injury • spinal cord compression syndrome • Upper extremity pathologies
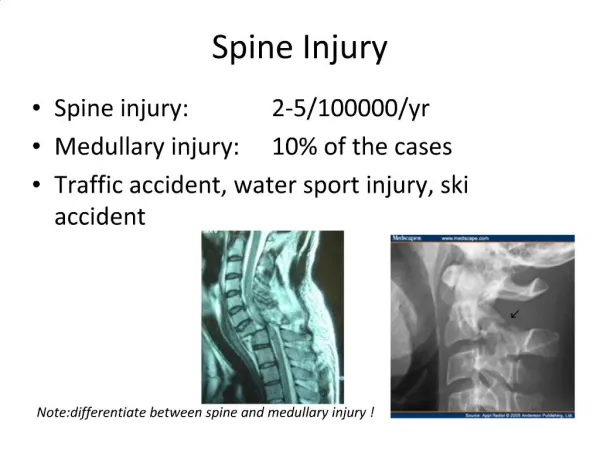
Diagnosis • Computerized tomography (CT) scan of his head, cervical, and thoracic spine revealed a C1 transverse process fracture, C5-7 posterior element fractures (including spinous process, lamina, pedicle, and pars), T1-3 burst fractures, and ribs 1-3 fractures, The rib fractures also caused a pneumothorax. • Later, he was diagnosed with left shoulder rotator cuff/long head biceps brachii tear and SLAP lesion.
Treatment • The first surgery was performed on July 2, 2008 (3 days post injury) for stabilization with a halo. Follow-up x-rays two days later revealed further instability of the T1-3 vertebral burst fractures. • A second surgery was performed on July 7, 2008 for external fixation of vertebral levels T1 through T5.
Treatment (cont.) • The subject started treatment with electrical stimulation and ice along the spine following the surgery. He started with ice the day of surgery and followed this course regularly (nearly continuously) for one month. • He began weight bearing and walking with minimal assistance two days post surgery.
Treatment (cont.) • He was discharged from hospital six days after the second surgery and after a total of two weeks in the hospital. • During week three, thoracic, scapular, and shoulder range of motion/resistive exercises (non-painful and safe for healing tissues) were initiated.
Treatment (cont.) • At four weeks post-operatively, when the dissolvable stitches were at their weakest, the subject reached forward and disrupted the surgical closure. • The wound became infected with Methicillin-resistant staphylococcus aureus (MRSA) bacteria and a third surgery and hospitalization was required for debridement and resuturing of the thoracic spine incision.
Treatment (cont.) • Early rehabilitation resumed four days post surgery with early mobilization of the shoulders and thoracic spine, gentle resistive upper extremity exercises, and daily walking of 30-90 minutes. • Follow-up x-rays at four weeks showed early bone regeneration. The halo was removed after 9 weeks since significant bone regeneration was present. • Cervical collar was removed after one week because of sufficient stabilization at the fracture sites
Treatment (cont.) • At 12 weeks, the subject returned to work 20 hours/week and cycling 6 hours/week. His daily rehabilitation regime consists active and passive range of motion, progressive resistance exercise with focusing on the upper extremities and cardiorespiratory conditioning
Treatment (cont.) • The subject still has C6 and C7 numbness and weakness four months post injury. However, EMG studies have demonstrated that the action potentials of the denervated nerves are regenerating. • Shoulder surgery was performed on 12/17/08 (biceps tenodesis, rotator cuff repair, labrum excision, and acromioplasty)
Today’s progress • Patient has regained approximately 80% of flexion and rotation. He has gained 70% of extension. He is limited in motion of upper thoracic spine due to fixation. • Left shoulder full ROM; strength @ 85% • Numbness still present around surgical incision. • Tidal volume decreased due to limited rib mobility.
Uniqueness • The principles for spinal trauma surgery are well documented. Rehabilitation strategies and techniques are more controversial. • Traditionally, patients are overmedicated and sedentary for the first two weeks post injury. Healing is slow and recovery of motion and strength difficult. • The typical recovery for an extensive spinal injury may take several years with only a small percentage regaining full function.
Uniqueness • Since the subject demonstrated early bone regeneration, the halo was removed in 9 weeks instead of the typical 12-16 weeks. The patient’s bone healed 30% faster than the typical cervical fracture patient. • At ten weeks, the subject was able to resume bicycle riding. At twelve weeks, the subject was back to working three half days a week as a physical therapist and had regained enough motion to drive a car.
Conclusion • Our subject’s rapid recovery was facilitated by an early rehabilitation, effective inflammation control, pre-injury level of fitness, and determination to regain function. • 10.5 months post-injury and four surgeries later, patient was able to return to high-level competitive cycling. He won the Washington State Omni Cycling Championship for masters over the age of 50.