Download

1 / 63
8.22k likes | 30.02k Views
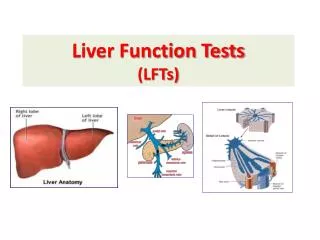
Liver function tests. ( LFTs ). xiaoli. Review: Liver. The liver is the largest organ in the body It is located below the diaphragm in the right upper quadrant of the abdominal cavity and extended approximately from the right 5th rib to the lower border of the rib cage.

E N D
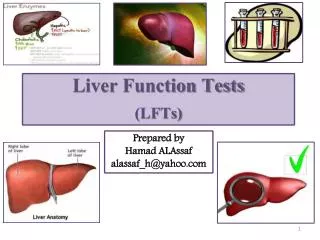
Liver function tests ( LFTs ) xiaoli
Review: Liver • The liver is the largest organ in the body • It is located below the diaphragm in the right upper quadrant of the abdominal cavity and extended approximately from the right 5th rib to the lower border of the rib cage.
The liver is separated into a right and left lobe, separated by the falciform ligament. The right is much larger than the left .
The liver performs an astonishingly large number of tasks that impact all body systems. • Liver have two channels that can supply and oxygen nutriment : hepatic artery and hepatic portal vein . • The corresponding channels is hepatic vein and bile ducts.
The working cells of the liver are known as hepatocytes, which have a unique capacity to reproduce in response to liver injury. • Liver regeneration can occur after surgical removal of a portion of the liver or after injuries that destroy parts of the liver. • Although the liver's ability to react to damage and repair itself is remarkable, repetitive insults can produce liver failure and death.
Functions of liver • Excretory function: bile pigments, bile salts and cholesterol are excreted in bile into intestine. • Metabolic function: liver actively participates in carbohydrate, lipid, protein, mineral and vitamin metabolisms. • Hematological function: liver is also produces clotting factors like factor V, VII. Fibrinogen involved in blood coagulation is also synthesized in liver. It synthesize plasma proteins and destruction of erythrocytes.
④ Storage functions: glycogen, vitamins A, D and B12,and trace element iron are stored in liver. ⑤Protective functions and detoxification: Ammonia is detoxified to urea. kupffer cells of liver perform phagocytosis to eliminate foreign compounds. Liver is responsible for the metabolism of xenobiotic.
Liver function tests ( LFTs )
What is Purpose of LFTs? • LFTs alone do not give the physician full information, but used in combination with a careful history, physical examination (particularly ultrasound and CT Scanning), can contribute to making an accurate diagnosis of the specific liver disorder. • Different tests will show abnormalities in response to • liver inflammation • liver injury due to drugs, alcohol, toxins, viruses • Liver malfunction due to blockage of the flow of bile • Liver cancers
LFTs are divided into • true tests of liver function, such as serum albumin, bilirubin, and protime, • tests that are indicators of liver injury or biliary tract disease.
Classification of liver functions test Classified based on the major functions of liver: • Excretion: Measurement of bile pigments, bile salts. • Serum enzymes: Transaminase (ALT, AST), alkaline phosphate(ALP), 5’-nucleotidase, LDH isoenzyme. • Synthetic function: Prothrombin time, serum albumin. • Metabolic capacity: Galactose tolerance and antipyrine clearance • Detoxification :
1. Excretion : Bilirubin • Bilirubin is the main bile pigment that is formed from the breakdown of heme in red blood cells. The broken down heme travels to the liver, where it is secreted into the bile by the liver.
Stercobilin excreted in feces Urobilin excreted in urine Hemoglobin Globin Urobilinogen formed by bacteria Heme O2 Heme oxygenase CO Biliverdin IX NADPH Bilirubin diglucuronide (water-soluble) Biliverdin reductase NADP+ 2 UDP-glucuronic acid Bilirubin (water-insoluble) Bilirubin (water-insoluble) LIVER via blood to the liver BLOOD CELLS KIDNEY reabsorbed into blood INTESTINE via bile duct to intestines Fig. 2 metabolism of bilirubin
1. serum bilirubin: • Normally, a small amount of bilirubin circulates in the blood. Serum bilirubin is considered a true test of liver function, as it reflects the liver's ability to take up, process, and secrete bilirubin into the bile. • A. indirect bilirubin (normal value = 0.3 - 1.2 mg/dl) • B. direct bilirubin (normal value ≤ 0.4 mg/dl) • C. total bilirubin Normal value for = 0.3- 1.2 mg/dl.
VD Bergh reaction ♣Direct Bilirubin + Diazotized Sulfanilic Acid → Azobilirubin (Redish purple) ♣ total bilirubin + dimethylsulfoxide(DMSO)+methanol +diazotized sulfanilic acid to form azobilirubin. Indirect bilirubin react with diazotized sulfanilic acidafter addition of methanol. The absorbance of the reaction mixture at 555 nm is directly proportional to the concentration of direct bilirubin.
OH COOH O O O OH OH HOOC CO CO O OH HO CH2 CH2 OH M M V M V M CH2 CH2 O CH CH O CH2 N N N N H H H H 目 录
2. urine(/faeces) • A. urobilinogen : Conjugated bilirubin is excreted via bile salts to intestine. Bacteria in the intestine break down bilirubin to urobilinogen for excretion in the feces (normal value for fecal urobilinogen = 40 - 280 mg/day) Normally there are mere traces of urobilinogen in the urine. average is 0.64mg , maximum normal 4mg/24hours. • B. Urobilin • Urobilin is the final product of oxidation of urobilinogen by oxygen in air. The amount change with the amount of urobilinogen excretion .
B. bilirubinurine: • Bilirubin is not normally present in urine and faese since bacteria in intestine reduce it to urobilinogen. The kidneys do not filter unconjugated bilirubin because of its avid binding to albumin. • conjugated bilirubin can pass through glomerular filter. • Bilirubin is found in the urine in obstructive jaundice due to various causes and in cholestasis. Note: Bilirubin in the urine may be detected even before clinical jaundice is noted.
Who is a candidate for the test? Bilirubin is used to diagnosis of jaundice. Abnormal bilirubin levels can be found in many disorders, including: blocked bile ducts, cirrhosis, hepatitis and other liver diseases or immature liver development in newborns. Hemolytic Jaundice Hepatic Jaundice Obstructive jaundice ( Cholestasis) Congenital Jaundice
2. Serum enzymes A large number of enzyme estimations are available which are used to ascertain liver function. They are be divided into two groups: I: most commonly and routinely done in the laboratory. serum transaminase(ALT/AST) serum alkaline phosphate(ALP) II: not routinely done in the laboratory.
GPT Alanine transaminase (ALT) • ALT or sGPT (serum glutamate pyruvate transaminase)
Aspartate aminotransferase (AST) GOT • AST or sGOT (serum glutamate oxaloacetate transaminase)
GPT GOT GPT GOT organ organ 2000 7100 156000 28000 heart pancrease 1200 142000 44000 14000 liver spleen 4800 99000 10000 700 skeletal lung 91000 19000 20 16 kidney serum GPT: Normal range: 2-59 U/L GOT: Normal range: 10-34 U/L
Therefore, when the liver is injured, GPT is released into the bloodstream. Elevated levels of GPT may indicate : • alcoholic liver disease • cancer of the liver • cholestasis or congestion of the bile ducts • cirrhosis or scarring of the liver with loss of function • death of liver tissue • Hepatitis or inflammation of the liver • noncancerous tumor of the liver • use of medicines or drugs toxic to the liver
GOT also reflects damage to the hepatic cells and is less specific for liver disease. It can also be released with heart, muscle and brain disorders. • Therefore, this test may be ordered to help diagnose various heart, muscle or brain disorders, such as a myocardial infarct (heart attack).
Elevated levels of GOT may indicate : • acute hemolytic anemia, • acute pancreatitis or inflammation of the pancreas. • acute renal failure or loss of kidney function. • cirrhosis of the liver. • Hepatitis • heart attack • primary muscle disease • recent surgery • severe burns • muscle injury
Although GOT is not a specific for liver as the GPT, ratios between GPT and GOT are useful to physicians in assessing the etiology of liver enzyme abnormalities. ◆ normally: GPT is normal, GOT is normal, GPT/GOT is about 1.15. ◆Virus hepatitis: GPT↑, GOT is normal ,GPT/GOT>1,even more than 2.5; ◆chronic hepatitis : GPT↑ ,GOT ↑GPT/GOT is about 1. ◆ Liver cancer, cirrhosis, Alcohol-induced hepatitis: GPT↑ ,GOT ↑ < 1, about 0.6~0.7. ◆ Accute myocardial infarct :< 1
GPT and GOT is in the different distribution of the hepatocytes. GPT exists primarily in the cytoplasm of liver cell. if there is a slight liver cell damage, GPT firstly leak into the bloodstream, so that the serum GPT increased. The GOT mainly in the "mitochondria“of liver cells, the mitochondria are "bubble" in the liver cell cytoplasm. if there is a slight liver cell damage, GOT don`t leak into the bloodstream. When the GOT was significantly higher, mitochondria of liver cells are injuries.
Alkaline phosphatase (ALP) ALP occurs in all tissues, especially liver and bone. The alkaline phosphatase test is often used to help diagnose certain liver diseases and bone disorders . Normal range: 30 - 95 IU/L (3-13 kings unit)
Alkaline phosphatase (ALP or AKP) • ALP is a hydrolase enzyme responsible for removing phosphate groups from many types of molecules, including nucleotides and proteins. • most effective in an alkaline environment • in humans, alkaline phosphatase is present in all tissues throughout the entire body, but is particularly concentrated in liver, bile duct, kidney, bone, and the placenta. • Levels are significantly higher in children and pregnant women.
Higher levels of ALP than normal may indicate: • liver disease • bone disease • leukemia, a cancer of the blood and bone marrow • various hormone problems • pregnancy Lower levels of ALP than normal may indicate: • anemia, or a low red blood cell count • malnutrition • various hormone problems
Mechanism of increase in ALP in liver disease: Increase in the activity of ALP in liver disease is not due to hepatic cell disruption , nor to a failure of clearance , but rather to increased synthesis of hepatic ALP . The stimulus for this increased synthesis in patients with liver disease has been attributed to bile duct obstruction by stone ,tumors , intrahepatically by infiltrative disorders or space-occupying lesions.
It is used for many years in differential diagnosis of jaundice. it is increased in both infectious hepatitis (viral hepatitis) and posthepatic jaundice, but the rise is usually much greater in case of obstructive jaundice . dividing line which has been suggested is 35KA units/ml. a value higher than 35KA units/ml is strongly suggestive of diagnosis of obstructive jaundice, in which very high figures even up to 200KA units/ml or more may be found. Serum ALP is found to be normal in haemolytic jaundice.
Other enzyme (not done routinely) 5’-Nucleotidase This enzyme is released by the liver when the liver is injured due to bile duct obstruction or impaired bile flow. Normal range: 2-15 IU/L
H H H H H H H H H M M M LDH1 (H4) LDH2 (H3M) LDH3 (H2M2) LDH4 (HM3) LDH5 (M4) H M M M M M M M LDH isoenzymes lactate dehydrogenase This test measures the total level of the enzyme lactic dehydrogenase, also called LDH, in the blood. LDH is found in body tissues and organs.
LDH isoenzymes ۩ Tissue or organ injury can release LDH into the bloodstream, thereby raising the level. So it is usually done to see if tissue or organ damage has occurred. ۩ If he or she suspects a heart attack or liver tissue damage in the body. Normal range: 115-225 IU/L
3. Metabolic capacity: Tests based on livers function: carbohydrate metabolism lipid metabolism protein metabolism
Tests based on livers part in carbohydrate metabolism 1. Glucose tolerance test &Not of much value in liver diseases &It is often difficult to separate the part played by the liver from other factors influencing glucose metabolism.
2. Galactose tolerance test Basis: For galactose is a monosaccharide, almost exclusively metabolized by the liver. the normal liver is able to convert galactose into glucose; but this function is impaired in intrahepatic disease and the amount of blood galactose and urine galactose is excessive. The liver can be assessed by measuring the utilization of galactose. This is referred to galactose tolerance test.
◆It is used primarily to detect liver cell injury. ◆It can be performed in presence of jaundice. ◆As it measured an intrinsic hepatic function, it may be used to distinguish obstruction and non obstruction jaundice.
Method : oral galactose tolerance test IV galactose tolerance test(intravenous injection ) The test is performed in the morning after a night’s fast. a fasting blood sample is collected which serves as “control”.40mg galactose dissolved in a cup-full of water is given orally.further blood samples are collected at ½ hourly intervals for two hours. oral galactose tolerance test
Result: Normally or obstructive jaundice: 3gm or less of galactose are excreted in the urine within 3 to 5 hours and the blood galactose returns to normal within one hour. Intrahepatic jaundice: The excretion amounts to 4 to 5gm or more during the first 5 hours.
3. Fructose tolerance test Normal response: shows little or no rise in the blood sugar level. The highest blood sugar value reached during the test should not exceed the fasting level by more than 30 mg%. obstructive jaundice cases: mresult is obtained in most cases of obstructive jaundice cases. In infectious hepatitis or parenchymatous liver cells damage: rise in blood sugar is greater than above, but the increases obtained are never very great.
Tests based on livers part in lipids metabolism Cholesterol-cholesteryl ester ratio: The liver plays an active and important role in the metabolism of cholesterol including its synthesis,esterification,oxidation and excretion. Normal total blood cholesterol ranges from 150 ~ 250mg/dl and approx 60 to 70% of this is in erterified form.
In parenchymatous liver disease: theer is either no rise or even decrease in total cholesterol and the ester fraction is always definitely reduced. the degree of reduction roughly parallels the degree of liver damage. In severe acute hepatic necrosis: the total serum cholesterol is usually low and may fall below 100mg/dl, whilst there is marked reduction in the % present as esters.
Tests based on livers part in amino acid metabolism Determination of blood NH3: Nitrogen part of amino acid is converted to NH3 in the liver mainly by transamination and deamination and it is converted to urea in liver only . Normal range : blood ammonia varies from 40μg ammonia nitrogen per100ml of blood. In parenchymatous liver disease: Increases in NH3 can be found more advanced cases of cirrhosis liver,particular when there areassociated neurological complicate.in such cases blood levels may be over 200 μg/ml.
4. Synthetic functions: 1. total plasma proteins/ albumin/ globulin/ A:G ratio 2. Formation of prothrombin by liver
1. Determination of total plasma proteins/ albumin/ globulin/ A:G ratio This yields most useful information in chronic liver disease.Liver is the site of albumin synthesis and also possibly of some of αand β globulins. Normal value: total plasma proteins: 80~110mg/dl albumin:40-50mg/dl globulin:25~35mg/dl A:G ratio: 1.5~2.5