Download
1 / 55
580 likes | 942 Views
Impact on Breastfeeding of Restrictive Lingual Frenulum. Dr David Edwards StR Public Health Public Health Suffolk. March 2012. Concern raised over access to infant ‘tongue-tie’ lingual frenulum (LF) division to support breastfeeding in Suffolk Investigation by Public Health :

E N D
Impact on Breastfeeding of Restrictive Lingual Frenulum Dr David Edwards StR Public Health Public Health Suffolk
March 2012 • Concern raised over access to infant ‘tongue-tie’ lingual frenulum (LF) division to support breastfeeding in Suffolk • Investigation by Public Health: • Ipswich Hospital - LF division policy and pathway in place • West Suffolk Hospital - did not provide LF division to support breastfeeding
NICE Guidance (2005) Division of ankyloglossia (tongue tie) for breastfeeding (IPG149) • Many ‘tongue-ties’ do not require treatment • Conservative treatment includes breastfeeding advice and counselling, exercising the tongue • Surgical division of the lingual frenulum may enable the mother to continue breastfeeding • Safe – if by competent health professional
East of England Picture • Over half of providers (n=8, 53%) with no policy/guideline for LF division • Seven providers with policies roughly in line with NICE IPG149 • Wide policy variation on assessment of LF and pathway followed
Its About Tongue Mobility! • Restricted tongue mobility can impair breastfeeding – Mother/infant interaction • Require clear identification, assessment of tongue mobility impact on breastfeeding • Intervention (LF division) when indicated • Risk of policy stimulating unnecessary LF division activity?
Regional policy Policy for Division of the Lingual Frenulum (tongue-tie division) of Infants (<3 months of age) to Support Breastfeeding • “..ensure consistency of approach in the East of England in the provision lingual frenulum division (tongue-tie division) where restricted tongue mobility due to a tight lingual frenulum is impairing the ability of the infant to breastfeed effectively”
Policy part 1: Assessment • BEFORE referral for division – competent health professional to assess tongue mobility • Is infant positioning and attachment correct? • Is tongue mobility impairing breastfeeding? • If it does not impair breastfeeding then division is not necessary
Policy part 2: Division • Who and where to divide LF that is impairing ability to breastfeed • Lingual frenulumis divided using sterile scissors • Safety • Suitable clinical room which meets infection control requirements • Two staff, clinician conducting division and assistant • Protocol in place for rapid response to uncontrolled bleeding
Policy Implementation • Training need for assessment of whether tongue mobility is affecting breastfeeding • Clear referral pathways across region for referral of infants identified with clinical need for LF division • Support for breastfeeding mothers who do not opt for division
Implementation of Policy:What needs to be done in Suffolk? • Training need for identification and assessment? • Where should mother and baby be referred to?
“Division of Restrictive Lingual Frenulum – why, when and where?” MrAshishMinocha Consultant Paediatric & Neonatal Surgeon, Jenny Lind Children's Hospital, Norfolk and Norwich University Hospital NHS Foundation Trust Dr David Edwards Specialist Registrar Public Health Suffolk County Council
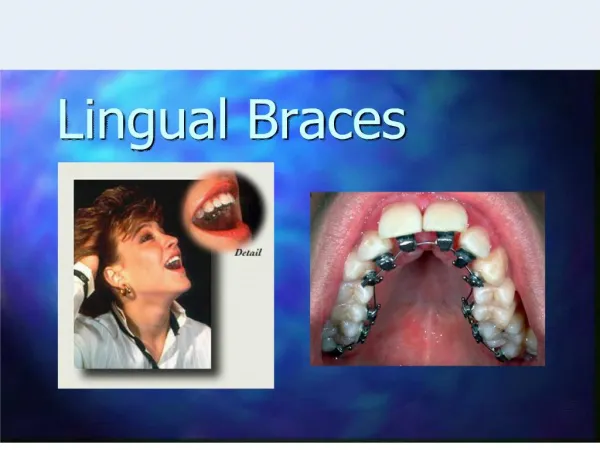
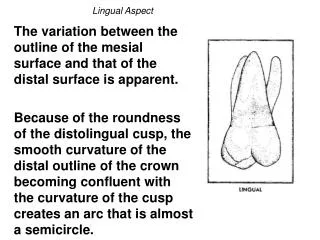
Lingual Frenulum • ‘Lingual frenulum' stretches from under the tongue to the floor of the mouth • Elastic and does not interfere with the movements of the tongue
Embryological origin • Vestigeal Structure • frenulum is what is left of the tissues that should have disappeared as the oral areas are formed • not uncommon • ‘webbing‘ can occur between upper or lower lips and gums, cheeks and gums as well as in at the base of the tongue
‘Tongue tie', ‘Ankyloglossia' or ‘short frenum' • Short Lingual Frenulum may lead to restriction of tongue movement
The Academy of Breastfeeding Medicine • defines partial ankyloglossia or “tongue-tie” as "the presence of a sublingual frenulum which changes the appearance and/or function of the infant's tongue because of its decreased length, lack of elasticity or attachment too distal beneath the tongue or too close to or onto the gingival ridge"
“Short, thick, tight or broad” Lingual Frenulum • Adverse effect on oromuscular function - feeding and ? speech • It may cause problems when it extends from the margin of the tongue and across the floor of the mouth to finish at the base of the teeth
Incidence • Variable • ?? Criteria • 1941 Study - 4 per 1000 of the population. • 16 percent of babies experiencing difficulty with breastfeeding had a tongue tie - University of Cincinnati, USA, 2002. • 10 % of the babies - SGH, UK.
Kotlow’s Criteria • With a finger, run it underneath the tongue from side to side. The feeling of a tie can be describe as a fence, speed bump or ridge in the bottom of the mouth. A normally developed mouth floor will feel smooth. Any kind of a bump has the potential to cause problems.
Genetic factors • Strong familial tendency or just an awareness ?? • Tongue tie sometimes occurs together with other congenital conditions which affect the structure of the mouth, such as cleft lip or palate. • It can also occur together with conditions such as severe hearing loss or cerebral palsy. • Boys are more often “tongue-tied” than girls !!
Diagnosis • Traditional criteria • Acute malnourishment • Mis-articulation of tongue tip sounds such as ‘t', ‘d', and ‘n'
Signs & Symptoms in Babies • Failure to latch on- slipping off the breast while feeding • continuous feeding - frequent & inadequate • Clickingsounds while feeding • Continuous Dribbling & gagging • Colic • “Windy baby” • Poor weight gain & physical growth
Maternal Signs & Symptoms • Sore nipples • Mis-shaped nipples • Mastitis and/or blocked ducts
Children, Adolescents & Adults • Appearance of the tongue • Lack of lingual mobility • speed and accuracy of tongue movements • Eating difficulties - poor coordination of oral musculature • Severe Dental problems • Unclear Speech ? • Inability to enjoy simple pleasures !!
Assessment • Breastfeeding, and any problems experienced • Measurements of ‘free tongue', and height to which the tongue can be lifted • Appearance of the margin of the tongue, and whether indentation is present • Function and ability to protrude or to elevate the tongue • Dental & Speech problems
Assessment & Classification • Kotlow assessment (American Paediatric Dentist) –length of free tongue>16 mm acceptable • Class I (12-16 mm) – mild • Class II (8-11 mm) – moderate • Class III (3-7 mm) - severe • Class 4 (<3 mm) - complete
Assessment & Classification • Hazelbaker Assessment tool • Lactational Consultant • Lingual Frenulum Anatomy & Function based assessment • rely on assessors judgement of appearance and any sucking problems
Reliability of the Hazelbaker Assessment Tool for Lingual Frenulum FunctionLisa H Amir, Jennifer P James and Susan M Donath, Melbourne, AustraliaInternational Breastfeeding Journal 2006, 1:3 doi:10.1186/1746-4358-1-3
Assessment & Classification • Appearance factors (Griffiths et al, Southampton) • diaphanous (transparent), • medium (non-transparent) • thick (chunky) • Visual assessment of the length • Digital Calliper Quantitative evaluation (Marchesan et al , Brazil) • Tongue tie Assessment Protocol (TAP) - scoring based on appearance and function
Consequences of Tongue Tie • Varied • Depends on age of presentation
Maternal challenges • The maternal experience of breastfeeding a tongue-tied baby may include: • Pain • Nipple damage, bleeding, blanching or distortion of the nipples • Mastitis, nipple thrush or blocked ducts • Severe pain with latch or losing latch • Sleep deprivation caused by the baby being unsettled • Depression or a sense of failure
Consequences in infants • Early problems with breast feeding may lead to • Termination of breastfeeding • Failure to thrive • Poor bonding between baby and mother • Problems with introducing solids
Consequences in Children • Inability to chew age appropriate solid foods • Inability to enjoy lollies / licking ice-creams • Dribbling, Gagging, choking or vomiting foods • Persisting food fads • Difficulties with dental hygiene/ Dental problems • ? speech problems • Behaviour problems • Lack of self confidence
Consequences in Adults • Consequences of un-repaired tongue tie may not reduce with time • Social, domestic and work environment difficulties • Lack of self-esteem • Dental health
Intervention • Before 1940, tongue ties were routinely cut to help feeding So what changed this practice ? • reduction in the practice of breastfeeding • “Not real medical problem” & “in the mind off over-zealous parents” • fear of excessive/unnecessary surgery
Intervention ? • Lactational Consultants & Breast Feeding Advisor • Struggling and suffering mums • And some of us starting to listen !
Tongue tie DivisionNeonates & Infants (prior to eruption of teeth) • Fax / email referrals accepted and encouraged to avoid delay. • Babies seen in next clinic – sometime on the same day of referral (majority within a few days to a week). • Office Procedure
Tongue tie DivisionNeonates & Infants • Procedure • One of the parent hold the baby • Usually cry when examining which helps in examination and division • Complete division of tongue tie • Some babies sleep through the procedure • Most stops crying as soon as handed over to mum and start feeding
Tongue tie DivisionNeonates & Infants • Tinge of blood – bleeding checked after 2 minutes and parents asked to wait another 20 minutes for a further review • Encouraged to report progress in 2 weeks via email / post or telephone • No follow up appointment
Response and Improvement All % rounded to the nearest whole number
Parental Satisfaction compared to Responses All % rounded to the nearest whole number