Download
1 / 46
540 likes | 1.52k Views
Paroxysmal Nocturnal Hemoglobinuria. March 8, 2005. Case. 43 y old Hispanic man who presented to his PCP for headaches. Labs revealed a pancytopenia. Referred to hematologist. Bone marrow revealed hypocellular marrow (5-10%).

E N D
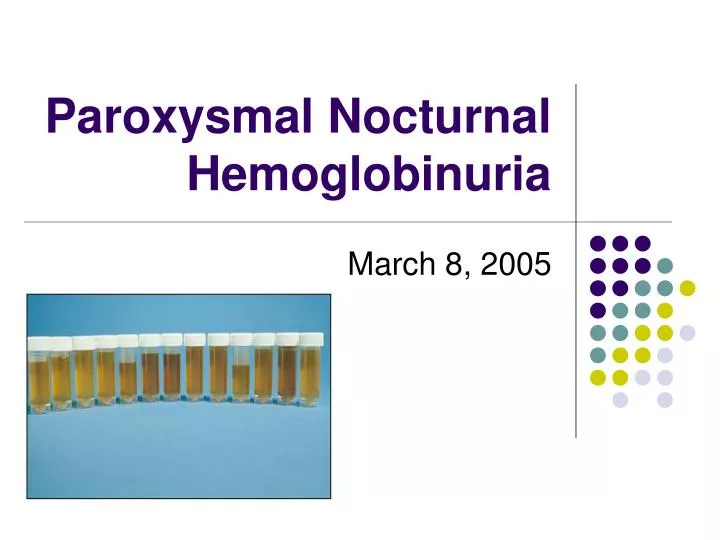
Paroxysmal Nocturnal Hemoglobinuria March 8, 2005
Case • 43 y old Hispanic man who presented to his PCP for headaches. Labs revealed a pancytopenia. Referred to hematologist. • Bone marrow revealed hypocellular marrow (5-10%). • Bone marrow repeated 6 months later showed minimally hypocellular marrow (30%). • Two years later, he developed dark urine and hemolytic anemia. • Bone marrow showed hypercellularity (80%) with normoblastic erythroid hyperplasia. A significant population of myeloid cells (85%) demonstrated atypically diminished expression of CD16, as well as an aberrant lack of CD55 and CD59 expression. A significant population of monocytic cells (83%) lacked expression of CD14, CD55, and CD59. • Findings consistent with PNH.
History • Investigator Year Contribution • Gull 1866 Described nocturnal and paroxysmal nature of “intermittent haematinuria” in a young man. • Strubing 1882 Distinguished PNH from paroxysmal cold haemoglobinuria and march haemoglobinuria. Attributed the problem to the red cells. • van den Burgh 1911 Red cells lysed in acidified serum. Suggested a role for complement. • Enneking 1928 Coined the name “paroxysmal nocturnal haemoglobinuria”. • Marchiafava 1928- Described perpetual hemosiderinemia. • and Micheli 1931 Their names became eponymous for PNH in Europe. • Ham 1937- Identified the role of complement in lysis of PNH red 1939 cells. Developed the acidified serum test, also called the Ham test, which is still used to diagnose PNH. Demonstrated that only a portion of PNH red cells are abnormally sensitive to complement. • Davitz 1986 Suggests defect in membrane protein anchoring system responsible • Hall & Rosse 1996 Flow cytometry for the diagnosis of PNH
Paroxysmal Nocturnal Hemoglobinuria • Described as a clinical entity in 1882. • Acquired disorder of hematopoiesis. • Triad: intravascular hemolysis, thrombosis, and decreased hematopoiesis. • “Nocturnal” refers to belief that hemolysis is triggered by acidosis during sleep and activation of complement to hemolyze abnormal RBCs. • However, hemolysis is shown to occur throughout the day and is not paroxysmal. Urine concentrated overnight may cause dramatic change in color.
Paroxysmal Nocturnal Hemoglobinuria • Due to an acquired hematopoietic stem cell mutation defect. • Somatic mutation (from deletions to point mutations identified) of the PIGA (phosphotidyl-inositol glycan class A) gene on the X-chromosome. Namely the transfer of N-acetylglucosamine to phosphatidylinositol. Hillmen and Richards, Br J Haematol, 2000
Paroxysmal Nocturnal Hemoglobinuria • Cells derived from the abnormal clone deficient in surface proteins normally attached to the cell membrane by a glycosylphoshpatidylinositol (GPI) anchor. • Essential group of membrane proteins lacking are called complement regulating surface proteins – decay accelerating factor (DAF) or CD55, homologous restriction factor (HRF) or C8 binding protein, and membrane inhibitor of reactive lysis (MIRL) or CD59. • These proteins interact with complement proteins and interfere with the assembly of complement's membrane-attack complex. • Deficiency CD59 is largely responsible for the hemolysis and implicated in the thrombotic tendency (induces platelet activation).
GPI Linked Proteins Rosti, Haematologica, 2000
GPI anchored Proteins Johnson and Hillmen,Mol Pathol, 2002
Paroxysmal Nocturnal Hemoglobinuria • Frequency: rate determined to be 5-10x less than aplastic anemia (2/million). Perhaps more frequent in Southeast Asia and Far East. • Men and women affected equally. • At any age, but frequently found among young adults. • Mortality/Morbidity: median survival of 10.3 yrs. Morbidity depends on variable expression of hemolysis, bone marrow failure, and thrombophilia. • Main cause of death is venous thrombosis followed by complications of bone marrow failure.
Hemolysis • Hemoglobinuria/hemosiderinuria. • Intravascular hemolysis - elevated retic count and LDH with low haptoglobin in the absence of hepatosplenomegaly. • Hemolytic anemia of variable severity: proportion of abnormal cells, degree of abnormality of the cells, degree of complement activation (viral or bacterial infections). • Bone marrow usually markedly erythroid with decreased iron stores. • Can be precipitated by administration of Fe to an Fe deficient patient due to large number of complement sensitive cells delivered to circulation at once.
Thrombosis • Hepatic vein (Budd-Chiari syndrome) – jaundice, abdominal pain, hepatomegaly, ascites. • Abdominal vein thrombosis – can lead to bowel infarction. • Cerebral vein thrombosis – if sagittal vein affected can lead to papilledema and pseudotumor cerebri. • Dermal vein thrombosis – raised, painful, and red nodules in skin affecting large areas. • Increased platelet aggregation, enhanced expression of tissue factor, and impaired fibrinolysis. • In two series, almost all patients developing thrombosis had more than 50% and 61% PNH granulocytes.
Cytopenias • Deficient hematopoiesis • Usually presents with anemia despite the presence of an erythroid marrow with suboptimal reticulocytosis. • Neutropenia and thrombcytopenia can occur in a hypoplastic bone marrow.
Other • Esophageal spasms can occur concurrently with episodes of hemoglobinuria. Manometry shows generation of peristaltic waves of great intensity. • Males can have impotence. • Absence of nitric oxide (taken up by hemoglobin in plasma)?
Abnormal Cells • PNH I cells normal in sensitivity to complement. • PNH II cells moderately more sensitive than normal cells (partial absence). • PNH III cells markedly sensitive, requiring one fifteenth to one twentieth of complement for an equal degree of lysis (complete absence). This group is increased in patients with more severe PNH and is associated with a mean life span of 10-15 days.
Diagnostic Test • Acid hemolysis (Ham test): PNH red cells incubated in separate tubes to fresh acidified serum (0.5mL), unacidified serum, and heated acidified serum. Lysis determined by optical density of the supernatant fluid after 1hr incubation and addition of 4mL of 0.15 M NaCl. • Positive test >1% lysis in acidified serum. • May be positive in congenitial dyserythro-poietic anemia • Specific but not very sensitive.
Diagnostic Test • The sugar water or sucrose lysis test uses the ionic strength of serum that is reduced by adding an iso-osmotic solution of sucrose, which then activates the classic pathway: sucrose molecules enter red cells through defects and produce osmotic lysis. • PNH diagnosed by >5% lysis. • Less specific but more sensitive.
Diagnostic Test • Low-tech test. The patient is asked to collect a sample of urine each hour for 48 hours. The physician lines them up and eyes their colors, and the diagnosis is plain.
Diagnostic Test • Flow Cytometry • Expression of GPI-anchored proteins CD55 and CD59 analyzed on hematopoietic cells using monoclonal antibodies and flow cytometry. • Highly specific. No other condition in which red cells are a mosaic of normal and GPI linked protein deficient cells.
Flow Cytometric Analysis Hillmen et al, NEJM, 1995
Pathogenesis • Relative/absolute bone marrow failure • present to some degree in all patients • relative granulocytopenia/thrombocytopenia • decreased capacity to form myeloid colonies • Two stage model • somatic mutation in PIG-A gene (understood) • some cause for bone marrow failure (not understood) • Is damage directed at a GPI linked molecule? • Mutant clone may expand as a result of an immune-escape from antigen-driven lymphocyte attack on hematopoietic progenitors.
Dual Pathogenesis Hypothesis Hillmen and Richards, Br J Haematol, 2000
Aplastic Anemia and PNH • The association between PNH and aplastic anemia goes both ways. • Although current emphasis is on patients with marrow failure who are found to have PNH clones, the older literature describes PNH patients with apparent progression to aplastic anemia. In such instances, the endstage has been called "spent PNH“. • All four of the following clinical scenarios are based on the same pathophysiologic mechanisms. The only difference is the temporal relationship between bone-marrow failure and somatic PIG-A mutation.
Natural History of PNH Hillmen et al, NEJM, 1995 • Long term study of 80 patients with PNH seen at one institution between 1940 and 1970 • Results • median age at diagnosis: 42 (16-75) • median survival: 10 years • 28% survived more than 25 years • 39% had one or more episodes of venous thrombosis • 12 experienced spontaneous clinical recovery • leukemia did not develop in any of the patients
Sites of Thrombosis in PNH Hillmen et al, NEJM, 1995
Natural History of PNH Hillmen et al, NEJM, 1995
Prognostic Factors • Thrombosis • Evolution to pancytopenia, myelodysplastic syndrome, or acute leukemia (1% ~ 10-100x more than normal) • Age >55 • Evidence of deficient hematopoiesis at disease onset, such as aplastic anemia or thrombocytopenia
Treatment • Supportive, prevent complement activation • Prednisone beneficial. Moderate doses (15-30 mg) administered on alternate days. Higher doses for acute episodes. • Fe supp given urinary loss (10-20x normal). Suppress hemoglobinuric episode with prednisone. • Folic Acid supp given increased need of hyperplastic marrow for cofactor. • pRBC transfusion as needed. • Androgenic hormones effective but mechanism unclear. • Eculizumab a monoclonal Ab that binds to C5 component of complement and inhibits terminal complement activation being studied.
Treatment • Therapy for/prevention of thrombosis • Thrombolytics acutely • Anticoagulation • First episode - managed as other patients with similar event • Recurrent episodes – lifetime • Prophylaxis – • Retrospective studies only, suggest warfarin prophylaxis effective in patients with PNH if the granulocyte clone size is >50%, platelet count >100K, no contraindications to ac. • Heparin or LMWH should be used in any perioperative period, during immobilization, or with use of indwelling intravenous catheter. Also start in 1st trimester of pregnancy until 4-6 weeks post-partum. • Efficacy of anti-platelet agents not clear.
Treatment • Stimulate hematopoiesis • G-CSF • Immunosuppression - hypothesis that immune-mediated bone marrow damage in PNH is primarily directed against the normal GPI-positive cells, producing growth advantage for PNH cells. Improved impaired hematopoiesis, but hemolysis and PNH clone not affected. • ATG • Cyclosporine
Treatment • Protein transfer – Transfer of GPI-linked proteins feasible using either high density lipoproteins or washed RBC microvesicles. PNH cells show increased cell-associated CD55 and CD59 levels and decreased hemolysis. • Gene Therapy - PIG-A gene cloned. But PIG-A inactivation alone does not confer a proliferative advantage to hematopoietic stem cell. Correcting the PNH defect may allow exposure to the insult causing bone marrow failure.
Treatment • Stem Cell Transplantation • Indications: severe bone marrow hypoplasia, severe thrombotic events (hepatic vein), children • Syngeneic (identical twin) – shown to be successful • Autologous - not very successful due to inability to obtain sufficient numbers of normal cells • Allogeneic • Allogeneic hematopoietic cell transplantation (HCT) after high-dose conditioning is the only curative treatment; however, it is associated with high treatment-related mortality.
Circulating Stem Cells in PNH Johnson et al, Blood, 1998
Stem Cell Transplantation in PNH • Summary of single institution trials • Approximately 12 reported • Number of patients ranges from 1-16 • Survival rates typically higher (58-100%) • Likely high degree of reporting bias, small studies
Stem Cell Transplantation in PNH IBMTR Data Saso et al, Br J Haematol, 1999
Results • Sustained engraftment: 77% • Graft failure: 17% • Grade 2-4 acute GVHD: 34% • Chronic GVHD: 33% • Causes of death: • graft failure (7), int. pneumonitis (4), GVHD (3), infection (3), ARDS (2), hemorrhage (1) IBMTR Data Saso et al, Br J Haematol, 1999
Stem Cell Transplantation in PNH Matched siblings IBMTR Data Saso et al, Br J Haematol, 1999
Stem Cell Transplantation in PNH • Conclusions from reported series: • BMT may cure 50-60% of selected patients with HLA-identical siblings • Most patients transplanted have been < 30 years of age • Regimen related toxicity and GVHD remain significant hurdles • Role of alternative donor transplants unclear, though initial reports are not encouraging except in pediatric population
Alternative Treatment • http://www.herbchina2000.com/therapies/HPH.shtml
Prognosis Based on Management Luzzatto, Haematologica, 2000
PNH: Management Guidelines Luzzato, ASH, 2001
Case • Started on prednisone, Fe, and Folate supplementation by Hematologist. • One year after diagnosed with PNH, patient admitted to PHD for pneumonia. WBC 2900 (ANC1800), H/H 11.7/33.6, plts 81,000 (labs one week prior normal CBC). LDH 2147, Tbili 2, Retic 3%. • Obtained records (bone marrow results) revealing diagnosis. • Prophylactic lovenox and higher dose prednisone given. Blood counts improved. • Did well. Discharged to f/u with his Hematologist.
References • Firkin, F, Goldberg, H, Firkin, BG. Glucocorticoid management of paroxysmal nocturnal hemoglobinuria. Australia Ann Med 1968; 17:127. • Rosse, WF. Treatment of paroxysmal nocturnal hemoglobinuria. Blood 1982; 60:20. • Hartmann, RC, Jenkins, DE Jr, Mckee, LC, heyssel, RM. Paroxysmal nocturnal hemoglobinuria: Clinical and laboratory studies relating to iron metabolism and therapy with androgen and iron. Medicine 1966; 45:331. • Saso, R, et al. Bone marrow transplants for paroxysmal nocturnal haemoglobinuria. Br J Haematol. 1999 Feb;104(2):392-6 • Risitano AM, et al. Large granular lymphocyte (LGL)-like clonal expansions in paroxysmal nocturnal hemoglobinuria (PNH) patients Leukemia. 2005 Feb;19(2):217-22 • Raiola, AM, et al Bone marrow transplantation for paroxysmal nocturnal hemoglobinuria.Haematologica. 2000 Jan;85(1):59-62
References • Moyo, VM, Mukhina, GL, Garrett ES, Brodsky, RA. Natural history of paroxysmal nocturnal hemoglobinuria using modern diagnostic assays. Br J Haematol 2004; 126:133. • Nishimura, J, Kanakura, Y, Ware, RE, et al. Clinical course and flow cytometric analysis of paroxysmal nocturnal hemoglobinuria in the United States and Japan. Medicine (Baltimore) 2004; 83:193. • Karadimitris, A, Luzzatto L. The cellular pathogenesis of paroxysmal nocturnal haemoglobinuria. Leukemia. 2001 Aug;15(8):1148-52 • Hillmen, P, et al. Natural History of Paroxysmal Hemoglobinuria. NEJM. 1995; 333 : 19. • Diagnosis and Treatment of paroxysmal nocturnal hemoglobinuria. UTD. • Clinical Manifestations of paroxysmal nocturnal hemoglobinuria. UTD. • http://hematology.im.wustl.edu/conferences/presentations/devine011703. • http://www.path.sunysb.edu/labs/pnh/PNH_files/frame.
References • Luzzatto L, Araten DJ. Allogeneic bone marrow transplantation for paroxysmal nocturnal hemoglobinuria.Haematologica. 2000 Jan;85(1):1-2