Download

1 / 71
720 likes | 1.25k Views
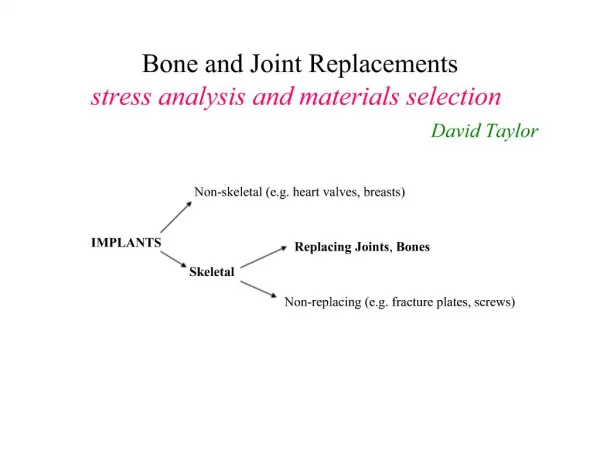
Joint Replacements. Causes: Trauma Osteoarthritis Reumatoid Arthritis Indication for Surgery Severe Pain Severe Deformation (knee in particular) Risks: Infection, Mechanical Failure (loosening etc.). Joint Replacements. The Joint Surface Problem (tribology) The lubrication problem

E N D
Joint Replacements • Causes: • Trauma • Osteoarthritis • Reumatoid Arthritis • Indication for Surgery • Severe Pain • Severe Deformation (knee in particular) • Risks: • Infection, • Mechanical Failure (loosening etc.)
Joint Replacements • The Joint Surface Problem (tribology) • The lubrication problem • Synovial fluid has to be the lubricant • Artificial joint does not employ the same hydrodynamic mechanism • How does a bearing work (hydrodynamics) • The wear debris and their consequences • The interface problem
Cartilage Shock Absorption of the Joint • Strictly essential in the lower limb joints, to protect the bone implant interface • Cartilage + Hydrodynamics in the Biological joint • Metal-UHMWPE (plastic)
Bone Disease: Osteoporosis Normal Bone Osteoporosis
Osteoporotic Femoral Head Normal Hip Osteoporotic Hip
Hip Fractures (From Howmedica) Over 250,000 hip fractures occur in the United States annually. 90% of these are in patients over 50 years old. With the growing aging population, the number of hip fractures is expected to double in less than 50 years. Types of hip fractures include: femoral neck fractures and fractures of the intertrochanteric and subtrochanteric regions. Femoral neck and intertrochanteric fractures occur with equal frequency and account for over 90% of all hip fractures. The remainder are subtrochanteric fractures. Treatment options range from internal fixation to total joint replacement.
Garden’s Classifications of Hip Fractures TypeI fractures have the best outcome. The bone ends are impacted into one another, which facilitates vascular re-growth.
OMEGA PLUS COMPRESSION FEMORAL SCREW SYSTEM The Complete System for Faster, Easier Surgery. The Omega Plus CHS System includes such features as sideplates made of superstrong alloy material, improved instrumentation, and the unique 98o ergonomically designed Supracondylar Plate which conforms to distal condyles with minimal contouring. Omega Plus plates and lag screws are available in sterile or non-sterile packaging for customer preference and convenience.
Hip Replacement If there is damage to the acetabulum the patient may require a Complete hip replacement.
Shock absorbing element Hip Joint Prosthesis
The Bone-Prosthesis Interface • Long stem in hip and elbow prostheses • Short stem in knee • Method of fixation • Acrylic bone cement • Simple contact (contour congruency) • Porous technology
Composite Beam (two materials) • For the beam to bend as one it should transmit shear • If one material is much more rigid it bears most of the stress • Preference in prosthetics is to have materials with rigidity similar to bone
Criteria to be Observed • Minimal bone removal • Mechanical compatibility (adjustment of compliance, Young’s moduli etc.) • Avoid stress concentration • Avoid stress shielding • Provide for easy extraction?? In case of revision surgery Anything else??
Simple fracture Displaced fracture Comminuted fracture Long bone fracture Vertebral fracture Rib fracture Clavicular fracture Pelvic fracture Radial fracture Finger fracture Fracture Fixation Examples of Fractures
Dynamic loading required Double plating may produce stress shielding Care is needed with the periosteum In some cases, compression plate is preferred Bone-Plate Fixation
In the epiphyseal region more screw support is needed Nail-Plate combination Bone Plates Cont.
Femoral nail vs. plating Intramedullary Nailing
Intramedullary Nailing http://www.smithnephew.com/orthopaedics/products.
Knee Arthrodesis The Knee Goes BadRadical Solution: Tibio-Femoral Fusion
Hoffman External Fixator Based on the long-standing tradition of the original Hoffmann Fixator, the new Hoffmann II design provides today's surgeon with advanced technology and ease of application. The new spring loaded snap fit mechanism allows the easy connection of 8mm connecting rods or pins providing versatile intraoperative frame management and excellent stability. The system allows independent pin placement of 4 or 5mm Apex Pins and is ideally suited for proximally or distally located fractures. The system is designed with versatile and simple instruments with a single wrench that fits all screws. A multi pin clamp is designed to accept the same pin placement as the original Hoffmann with single or bi-lateral torx connections allowing 12 angular positions for a compact frame design. http://www.howmedica.com/
Monotube External Fixator http://www.howmedica.com/
Fracture Fixation http://www.howmedica.com/
Arm Fractures Fixation Bridging Radial Fracture http://www.howmedica.com/
Pelvic Fracture External Fixation
Bioresorbable Materials Stimulan™, medical grade calcium sulfate dihydrate and stearic acid, is an osteoconductive material used to fill bone voids in non weight bearing applications that resorbs and is replaced with bone during the healing process. Stimulan is indicated for uses in cases where there is a bony defect or void in the boneTraumaSpinal fusions Revision SurgeryInfected JointsCore DecompressionsOsteoporosis Advantages of Stimulan: Predictable, consistent resorption ratesEliminates need for second surgical site and added pain for patient that occurs with traditional autograft techniqueCost and time savings per procedure over autograftOsteoconductive material that acts as scaffolding for new bone to formEliminates risk of disease transmission and availability of quality bone present with traditional allograft techniqueProven dissolution rates