Download
1 / 76
770 likes | 1.24k Views
Prof. Liu Jianhua PhD. MS. DDS. Dept. of Oral-Maxillofacial Surg. & Dentistry First affiliated hospital Zhejiang university school of medicine. Tumors in oral & maxillo-facial region. Naming : original tissue, biological type, position. Such as: squamous cell carcinoma of right tongue

E N D
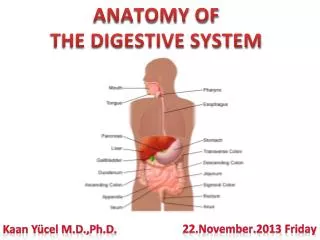
Prof. Liu JianhuaPhD. MS. DDS.Dept. of Oral-Maxillofacial Surg. & DentistryFirst affiliated hospitalZhejiang university school of medicine
Tumorsin oral & maxillo-facial region Naming:original tissue, biological type, position. Such as: squamous cell carcinoma of right tongue Critical t. :biologically benign tumor, but has malignant tendency and infiltrating growth. such as:ameloblastoma, mixed tumor, papiloma.
A mass in left submandibular region for 5 years, slow growing, with no symptom. Diagnosis? Further examination?
Left tongue ulcer 3 months, painful, Poor condition of oral cavity, what to do next?
Black lesion in soft palate, grows rapidly recent 3 months, shall we make a biopsy?
manifestations & diagnosis Judgement of a mass on patient : 1)tumor / not tumor(inflam. TB, malformation, etc.) 2)benign / malignant
Differentiation benign tumor malignant tumor Age any age carcinoma/agedness;sarcoma/young Growth speed slow faster Growth manner bulge invasive Boundary smooth,movable unclear,unmovable Symptom generally no painful/numbness/funct.limmit Metastasis no maybe Body affectgenerally no organ destroy/system destroy Histology struct. well differentiated worse diff./abn. nuclear close to norm.cell/tissue division;
Means of diagnosis 1)case history:arise,progress 2)clinical examine:look、touch、 listen to(with stethoscope ) 3)image:X-ray,panoramic radiograph,CT,MRI, DSA,B-ultrasonic,PET/CT 4)puncture:for liquid 5)biopsy:no melanoma/parotid g. 6)tumor markers:CEA, AFP, CA50/125/153/242/724 etc.
treatment 1)treatment principle:benign tumor—surgery first;malignant t.—combined 2)methods : Surgery.:safe edge—1 cm for malignacy Radiotherapy.:oral preparation—remove ill tooth and metal crown; fill decayed tooth; tooth cleaning---(to prevent jaw infection, necrosis, redial beam focus) Chemotherapy:before,during, post-operation others:thermotherapy./immunother. /herbs/ biotherapy
Prevention of oral cancer eliminate or reduce carcinogen:incomplete tooth root or crown、displaced tooth、sharp tooth edge、poor denture;hot food、tobacco and alcohol;environment contamination(air pollution,paint,glue);psycho-problem. treat precancerous lesion in time:mucosa erythema、leukoplakia 、oral lichen planus 、papilloma etc. investigate vulnerable population and give education
Commonness of Cysts囊肿共性 有囊壁wall、囊内容物content(液体/固形物liquid/solid) 边界清楚 缓慢增大 颌骨囊肿可造成骨组织压迫性吸收expansile absorbing
软组织囊肿一、皮脂腺囊肿sebaceous cyst • 病因pathogeny:皮脂腺sebaceous gland排泄管阻塞,分泌物蓄积----潴留性retentive囊肿。 • 临床表现:与皮肤粘连。色素点pigment dot。恶性变----皮脂腺癌。 • 治疗:梭形shuttle切口--疤痕。二次法(刘氏)
二、皮样、表皮样囊肿dermoid / epidermoid cyst • 病因: 胚胎embryo期上皮残留remnant、后天植入(手术、外伤) • 临床表现:青少年。皮样----口底、颏下。表皮样----面部。与皮肤无粘连。面团样----上皮细胞、毛囊、毛发、皮脂腺。 • 治疗: 手术摘除。下颌舌骨肌、颏舌骨肌----上、下进路不同。
三、甲状舌管囊肿thyroglossal tract cyst • 病因:胚胎第四周----甲状腺始基----甲状舌管----第六周:管消失,留下甲状腺、舌盲孔。管残留----囊肿。下移障碍----异位甲状腺。 • 临床表现:1-10岁>成年。 舌盲孔----胸骨切迹之间。舌骨上下最多。圆形,质中,囊性感,随吞咽、伸舌运动,穿刺----无色/有色液体,B超。感染----瘘----癌变。
(鉴别诊断) 舌异位甲状腺:舌根部,蓝紫色,柔软,“含橄榄”音。 1、迷走甲状腺:除异位外,颈部无甲状腺。 2、副甲状腺:颈部也有,舌根也有。 * 碘-131/锝-99扫描为可靠依据。 • 治疗 囊肿+舌骨中段一起切除。 误切迷走甲状腺----终身服药。
四 鳃裂囊肿branchial cleft cyst • 病因: 胚胎第三周----5对鳃弓----4对鳃裂----鳃裂上皮残余----囊肿 • 临床表现: 20-50岁(第一鳃裂年龄较小)。质软,波动感fluctuate,上呼吸道感染----增大,恶变----鳃裂癌,感染----鳃裂瘘fistula(有外口无内口),先天瘘congenital----原发性鳃裂瘘(有外口也有内口),穿刺----有色/无色;含/不含胆固醇液,B超。
二、颌骨囊肿maxillary cyst • 牙源性颌骨囊肿odontogenic jaw cyst 造牙组织/牙----演变而来(根尖、含牙、角化、始基) • 非牙源性颌骨囊肿non-odontogenic 胚胎期面突残余上皮----面裂囊肿 创伤----血外渗性囊肿intra-bleeding
牙源性颌骨囊肿odontogenic jaw cyst • 根尖囊肿(radicular cyst) 慢性根尖周炎----肉芽肿----牙周膜上皮残余----上皮团块----液化 残余囊肿(residual cyst):拔牙后肉芽肿残留所致
始基囊肿 (primordial cyst) 造釉器发育早期----星网层变性----渗出 • 含牙囊肿 (dentigerous cyst) 牙冠表面与缩余釉上皮之间----渗出 • 角化囊肿 (keratocyst) 原始牙胚/牙板残余----增生(含角化物,壁厚,子囊/上皮岛)
临床表现clinical characteristics 缓慢、膨胀性生长----颌骨坚硬肿块----乒乓感----波动感----骨折
诊断 • 穿刺 草黄色液体 • X线 根尖囊肿----根尖在囊内,死髓 始基囊肿----下8区/升支部好发 含牙囊肿----牙冠在囊内 角化囊肿----下8区/升支部好发
治疗 • 手术摘除 局麻/全麻,口内/口外 角化囊肿易复发/癌变:石炭酸/硝酸银腐蚀骨壁 死腔消除
第三节 良性肿瘤和瘤样病变benign tumor & tumor-like lesion • 口腔颌面部软/硬组织内的良性、实质性、占位性病变,生长缓慢(一般以年为单位)。
色素痣nevus • 皮肤构成:图示 • 色素痣起源:基底层黑色素细胞团。 • 皮内痣---真皮内,分化高的小痣细胞团,如雀斑样。 • 交界痣---表皮真皮交界;大痣细胞;可恶性变---恶黑。 • 复合痣---表皮+真皮;大痣+小痣细胞,如毛痣。
牙龈瘤(epulis) • 病因:机械/慢性炎症刺激---牙龈肿块(非真性肿瘤) • 肉芽肿型---炎症细胞+毛细血管为主,易出血 • 纤维型---纤维组织+纤维母细胞,不易出血 • 血管型---似血管瘤,极易出血(妊娠性龈瘤) • 治疗原则: 易复发---去除病变+牙+邻近骨组织
(一)、成釉质细胞瘤(ameloblastoma) • 多数人认为由造釉器或牙板上皮发生而来。剖面实质性(多)/囊性(褐色液),或混合。 • 临床表现:青壮年多,下颌体/角多,缓慢增大,大到一定程度----各种临床表现(牙、骨、神经受累)。可恶变(少)。 • 诊断:X片:蜂房状----多房性囊肿样阴影,边缘不齐,半月型切迹,根尖吸收。 • 治疗:易复发,须在边界外0.5cm切除。植骨准备。 • 问题:成牙釉质细胞瘤有那些临床特点?
hemangioma 血管瘤 • 1) authentic tumor • 2) account for 60% of body hemangiomas • 3) head vs.body? 1:9? • 4) most disappear before 10 year-old • 5) surgery or not?
Clinical characteristics • 1) newborn—strawberry like on skin • 2) rapid growth—after 1 month • 3) stillness or shrinking—after 1 year • 4) disappear—50-60% within 5 year; 75% within 7 year; 90 % within 10 year. • 5) end of disappear—10-12 year • Question: shall we recommend surgery? • Advantage ? Disadvantage?