Download

1 / 10
100 likes | 226 Views
NHS Budgets 2011/12. Alan Campbell – NHS Salford. Introduction. National Policy for Health Organisational change Quality Innovation Productivity and Prevention (QIPP) Salford Service impact. April 2011 > PCTs merged into Clusters (10>1 GM) April 2011 > GP Commissioning Pathfinders active

E N D
NHS Budgets 2011/12 Alan Campbell – NHS Salford
Introduction • National Policy for Health • Organisational change • Quality Innovation Productivity and Prevention (QIPP) • Salford Service impact
April 2011 > PCTs merged into Clusters (10>1 GM) April 2011 > GP Commissioning Pathfinders active April 2012 > SHA abolished April 2012 > Health & Well Being Boards April 2012 > National Commissioning Board April 2013 > PCTs abolished April 2013 > Public Health statutorily LG responsibility April 2013 > GP Commissioners statutory Orgs National Policy for NHS
Challenge for PCTs • Reducing Real Time Resources - £ • Technology & New Drugs Emerging • Population Health issues • Tobacco • Alcohol & Drugs • Obesity • Lifestyle • Consumer access ‘free service’ issues • Eg Bariatric Surgery
National Context Funding Growth ‘c. 0.1% growth next 3 years v 5.2% 10/11 Uniqueness of Health Care inflation Reducing Management Capacity Developing GP Consortia Local Government Funding Reductions
State of The Local Health System Health Slow improvement to mortality/morbidity indices Poor Cancer outcomes The Indicators A&E attendances increasing Outpatient (new) slowing Outpatient (F/up) accelerating Urgent Admissions increasing (fast!) Elective work volumes stable Prescribing – High volumes but improving cost effectiveness The system approach Integrated (Urgent) Care Work Community Services Transformation GP Commissioning now well under way Finances Relatively stable now But Pressure Building!!
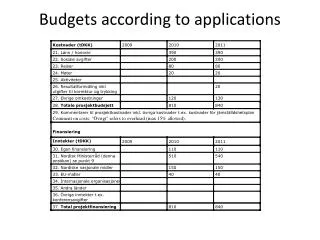
Specific Areas For Cost Reductions Hospital Services - £16M annually for 4 years (£64M) Urgent / Unscheduled Care - £7.2M in 3 years Community Services – c£5M in 4 years Drug Budgets - £8M in 4 years Management Costs - £5M in 3 years Total c £90M in 4 years
What it means for patients • C 15% real terms reduction in NHS expenditure • Greater choice over treatment ‘no decision about me without me’ • Greater involvement (co-production) with the public including determining priorities • Leaner ‘back office’ • More focus on prevention & early intervention • Supporting individuals & communities to manage own health better • Health promotion and education at every opportunity • Doing what's most cost effective (Prevention is a better investment than treatment)
Economics of Health Care • Techniques to measure health benefit • Quality Adjusted Life Years (QALY) • Treatment of end stage Diabetes Very expensive • Need to understand cost effectiveness of: • Prevention: • Lifestyle interventions c £11,600 QALY • Metformin c £15,000 QALY • Screening • Blood Lipid Secondary Prevention c £22,000 QALY • Retinopathy screening c £17,000 QALY • Hospital Treatment • Hospital Dialysis c £30,000 QALY • Erythropoietin (EPO) c £50,000 QALY • Disability and Social Economic Costs !