Download

1 / 51
520 likes | 718 Views
Emotional wellbeing of women living with HIV. Women for Positive Action is supported by a grant from Abbott. Contents. Introduction and evidence base. Emotional challenges and triggers. Depression. Suicide, trauma, PTSD. Stigma. Psychosexual wellbeing. Parenthood, pregnancy and menopause.

E N D
Emotional wellbeing of women living with HIV Women for Positive Action is supported by a grant from Abbott
Contents Introduction and evidence base Emotional challenges and triggers Depression Suicide, trauma, PTSD Stigma Psychosexual wellbeing Parenthood, pregnancy and menopause Treatment Case studies Women for Positive Action is supported by a grant from Abbott
Introduction and evidence base Women for Positive Action is supported by a grant from Abbott
Introduction Adjusting to treatment and living with HIV Diagnosis and coping Care and relationships • HIV infection can be both: • Chronic • Acute and life-threatening • HIV is associated with significant ‘emotional health’ challenges Women for Positive Action is supported by a grant from Abbott
Social and cultural differences affect how women manage HIV More limited scope to negotiate frequency of and nature of sexual interactions More limited power/control to practice low-risk sexual behavior Violence may increase a woman’s vulnerability to HIV Migrant women, in particular, are often isolated and lack social support Simultaneous management of medications, jobs, families and other medical and gynecologic problems is challenging Language or cultural barriers may add to lack of support Impact of religious and cultural beliefs on women Reduced access to healthcare, education and economic resources May come from ‘hard to reach’ communities 5 Women for Positive Action is supported by a grant from Abbott
Positive emotional health • Positive emotional health and wellbeing among women living with HIV promotes: • coping with diagnosis/HIV status • adjusting lifestyle to suit treatment • resilience to stigma/disease • Studies have shown that counselling and cognitive-behavioural interventions (both group and one-to-one) contribute to a reduction in distress and an increase in overall quality of life1 • Counselling has also been shown to be very effective in promoting positive emotional health and wellbeing and also reducing HIV risk behaviours2 • Peer support and mentoring is useful for many women, particularly those in whom there may be cultural and social barriers to medical counselling Women for Positive Action is supported by a grant from Abbott
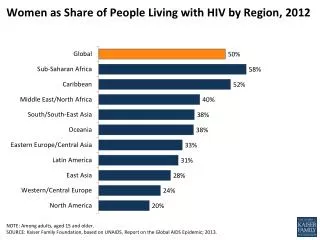
Emotional health in women with HIV • Globally women account for ~50% of HIV infections • Lack of data on the impact of HIV on women • Particularly psychosocial/emotional health issues • Historically research has focussed on: • Men, in particular men who have sex with men • Intravenous substance users • Limited studies and surveys have revealed some interesting gender differences1 Women for Positive Action is supported by a grant from Abbott
Published studies of the impact of HIV on emotional health of women Women for Positive Action is supported by a grant from Abbott
Emotional challenges and triggers Women for Positive Action is supported by a grant from Abbott
HIV often has mental and emotional consequences Relationships, independence, violence Parenting, pregnancy, children, carer resposibilities Quality of life Diagnosis-related trauma Coping, adjustment, responding to treatment Challenges for HIV-positive women Stigma-related stresses, fear, secrecy Disclosure-related stresses Ageing and the menopause Depression, suicidal thoughts /acts, emotional stress Risk behaviours Grief, loss and guilt Body image problems Women for Positive Action is supported by a grant from Abbott
How women experience HIV: the patient journey + Acceptance / moving on Starting treatment Disclosure (often avoided) Pregnancy, job loss, negative life events (at any stage) Improvement in emotional wellbeing Side effects If rejected by loved ones If rejected bypartner Denial Depression(can continue) Diagnosis - optimal journey emotional disturbance and depression The journey is characterised by many emotional ups and downs and varies from woman to woman. It adheres to the classic grieving model The Planning Shop International Women Research, July 2008 11
Emotional triggers in HIV 12 Women for Positive Action is supported by a grant from Abbott
Specific triggers for emotional disturbance in HIV 13 Women for Positive Action is supported by a grant from Abbott
Depression Anxiety Coping problems Suicidal thoughts and actions Trauma Post-traumatic stress disorder (PTSD) Neuro-cognitive impairment Stigma Psychosexual problems Relationship issues Pregnancy Menopause Body image Confidence Range of emotional health issues associated with HIV Women for Positive Action is supported by a grant from Abbott
Depression Women for Positive Action is supported by a grant from Abbott
Vulnerability of HIV-positive women to depressive symptoms • 17% higher likelihood of acute stress disorder among women compared with men2 • 30–60% of women with HIV in the community and clinic samples report depression1 • 54% HIV-related mortality rate for women with chronic depressive symptoms1 compared with little or no depressive symptoms • Some ART drugs and regimens are associated with a higher prevalence of depressive symptoms4 • 34% of women diagnosed with depression compared with 29% of men3 16 Women for Positive Action is supported by a grant from Abbott
Reduced adherence to HIV therapy in depression • Women with HIV and depression are significantly less adherent to therapy compared with HIV-positive men P=0.001 30 25 25 18 20 % of adherence to therapy 15 10 5 0 HIV + women HIV + men Turner BJ et al (2003) J Gen Intern Med Women for Positive Action is supported by a grant from Abbott
Improved survival associated with adherence to treatment Lima VD et al (2007) AIDS Women for Positive Action is supported by a grant from Abbott
Reduced risk behaviour following intervention 12 months 6 months 0 % reduction in new STDs diagnosed –5 –10 –15 –20 –20%* –25 –30 –30%* • Counselling may reduce risk behaviours *P<0.05 for counselling vs. didactic messages Kamb ML et al (1998) JAMA Women for Positive Action is supported by a grant from Abbott
Suicide, trauma and post-traumatic stress disorder (PTSD) Women for Positive Action is supported by a grant from Abbott
High level of suicidal ideation in HIV-positive women • Predictors of suicidal ideation and attempts include: • HIV diagnosis • Other psychiatric symptoms • Physical/sexual abuse • Drug/alcohol history • Isolation • People attempting or considering suicide often do not ‘seek death’ but simply cannot ‘face life’ Women for Positive Action is supported by a grant from Abbott
Suicide prevention strategies: need to be implemented immediately after diagnosis • React to suicidal ideation and comments • Ensure access to support and services such as crisis centres • Encourage woman to make plans for the future • Treat depression, alcohol/substance use disorders • Encourage friends and family to restrict access to common methods of suicide and situations with a high suicide risk • Teach cognitive coping strategies • Encourage a spiritual connection Women for Positive Action is supported by a grant from Abbott
Link between trauma and HIV • HIV patients often report a history of trauma e.g. a previous sexual assault or abuse1 • Severe traumatic events include:2 • Physical or mental abuse • Parental neglect • Death of a spouse • Trauma and abuse are linked with:1 • Unsafe sex and other high-risk behaviour • Poor adherence • Higher levels of mental illness Women for Positive Action is supported by a grant from Abbott
Post-traumatic stress disorder (PTSD) in women with HIV • 16–54% of HIV patients suffer from PTSD1 • PTSD is positively associated with female gender2 • Women at risk of PTSD are more likely to have experienced traumatic events3 e.g.: • Childhood sexual abuse1,3 • Severe physical abuse1,3 • Depression and PTSD often co-occur4 • PTSD is associated with1: • Poorer medication adherence • HIV risk behaviour Women for Positive Action is supported by a grant from Abbott
Stigma Women for Positive Action is supported by a grant from Abbott
HIV-related stigma Stigma is defined as an: “attribute of an individual that is undesirable or discrediting in the eyes of society, thus reducing that individual’s status” Perceived Directly experienced Linked with depression, PTSD, increased risk behaviour Associated with poor medication adherence Women for Positive Action is supported by a grant from Abbott
HIV-related stigma in women • In some cultures, HIV-positive women are treated differently than men • Effects of HIV-related stigma include: • Loss of income and carer options • Loss of marriage, partnership and procreation options • Poor care within the health sector • Rejection from family/friends (social rejection) • Loss of hope and feelings of worthlessness • Loss of reputation • Exclusion from religious/cultural communities • Violence Women for Positive Action is supported by a grant from Abbott
Psychosexual wellbeing Women for Positive Action is supported by a grant from Abbott
Impact of HIV on psychosexual wellbeing HIV Sex Safer sex Relationships • Safer sex practice • Commitment to condom use • Non-penetrative sex • Control • Disclosure, • rejection and • acceptance • Concordance/ • discordance • Relationship strategies • Interest in sex • Sexual enjoyment • Changing sexual behaviour Women for Positive Action is supported by a grant from Abbott
Common psychosexual problems reported by HIV-positive women % HIV-infected women Sonnenberg-Schwan U, 10th European AIDS Conference 2005 Women for Positive Action is supported by a grant from Abbott
Factors contributing to sexual dysfunction in HIV-infected women Psychogenic factors Organic factors Anxiety Fertility issues Relationship issues Treatment related Economic Cardiovascular disease Loss of partner Lipodystrophy/ Body image Depression Drug abuse Neurological impairments Guilt/shame Grief reactions Endocrine problems Pregnancy Fear of infecting others Sexual/physical abuse Socio-cultural Other issues e.g. surgery, radiotherapy Infective causes Lack of sexual desire Women for Positive Action is supported by a grant from Abbott
Parenthood, pregnancy and menopause Women for Positive Action is supported by a grant from Abbott
Influence of HIV on a woman’s role as a mother • Parenting issues for women with HIV • Disclosure to children • Confidentiality • Guilt/shame • Fear of passing infection to children • Caring for children with HIV • Adhering to complex treatment regimens • Stress of logistics of attending medical consultations • Managing childcare during periods of ill health • ‘Aftercare’ of children in the event of death • Migration • Family illness and other caring responsibilities • Secrecy around HIV Women for Positive Action is supported by a grant from Abbott
Disclosure to children • The decision to disclose HIV serostatus to one’s children is very complex • Rates of disclosure range from 30% to 66% • Possible concerns of disclosure include not wanting to scare the child, and wishing a care-free childhood for him/her • Benefits of disclosure may include: • opportunities to openly discuss the diagnosis and any concerns the child may have and to clarify misconceptions • providing the child with time to grieve • opportunities for the mother to gain comfort from her child Delaney RO et al (2008) AIDS Care Women for Positive Action is supported by a grant from Abbott
Concerns for pregnant HIV-positive women HIV diagnosis during pregnancy HIV diagnosis during pregnancy Development of major depressive/ somatic illness Need for rapid decision-making Balance joy of pregnancy with news of diagnosis Experience surrounding diagnosis Expectation and preparation Possibility of abortion? HIV diagnosis before pregnancy Fertility treatment Discordant partner Baby’s HIV status Treatment effects Giving birth Feeding baby Women for Positive Action is supported by a grant from Abbott
Addressing depression in pregnancy Guidelines should be updated to recommend Preconception counselling Guidance on reproduction options Identify modifiable factors associated with prenatal depression Integrate routine screening into prenatal HIV-care Enhancing education to lower depression rates Reduces perceived stress and social isolation Encourages positive partner support Alleviates fear over treatment effects and adherence concerns Offer access to peer support networks Women for Positive Action is supported by a grant from Abbott
HIV in menopausal women • Due to improved therapies many HIV-positive women now survive to experience menopause1 • 24–65% increased likelihood of experiencing symptoms in menopause with HIV2,3 • Commonly reported symptoms include: • Depression • Reduced sexual interest2,3 • Lower CD4 cell count is significantly associated with hot flushes/night sweats4 Women for Positive Action is supported by a grant from Abbott
Hormone replacement therapy (HRT), HIV and ART • Studies investigating the relationship between HIV, ART and menopausal symptoms are limited • Age at menopause is unaffected by ART1 • No available evidence supporting safe use of HRT in HIV patients • Studies of the safety and efficacy of HRT in HIV-positive women should consider potential drug-drug interactions with ART Women for Positive Action is supported by a grant from Abbott
Treatment Women for Positive Action is supported by a grant from Abbott
Treating emotional health problems to improve health outcomes • Decrease treatment costs • Improve QOL • Improve access to psychological services Emotional health services • Reduce stigma • Reduce distrust Specialisteducation • Improve medication adherence • Reduce risk behaviour Patient education and peer support Women for Positive Action is supported by a grant from Abbott
Individualizing care Socio-economic class Age Family issues Sexual issues Medical history Treatment should vary depending on the unique needs and personal circumstances of each woman . . . Pregnancy Support Stage of HIV journey Immigration Child-bearing potential Violence or sexual abuse Co-morbid problems (e.g. alcoholism, drug use, depression) Acceptance of diagnosis Culture or religion Language and understanding Women for Positive Action is supported by a grant from Abbott
Individualizing care . . . and consider women in their social contexte.g. as a mother, a partner, a daughter, a caregiver Women for Positive Action is supported by a grant from Abbott
Case studies Women for Positive Action is supported by a grant from Abbott
Case study 1: HIV-positive mother coping with diagnosis HIV-positive mother, diagnosed during pregnancy who did not share her status with any of her family Child’s father left soon after the birth Mother shows signs of depression and mood disturbance She claims not to have suicidal thoughts but mentions wanting to ‘disappear’ and feeling life is ‘pointless’ In addition to managing her diagnosis and following up on the baby’s health, what other issues should be considered? 44 Women for Positive Action is supported by a grant from Abbott
Issues to consider Mental health and emotional wellbeing Women are more likely to be diagnosed with mental health and emotional problems than men Pregnancy increases the risk of emotional or family problems in HIV positive women HIV diagnoses made during pregnancy are associated with a higher incidence of mental health issues, e.g. post-partum depression, than non-pregnancy diagnoses1 Not all HIV clinics have good access to perinatal psychiatric services 45 Women for Positive Action is supported by a grant from Abbott
Issues to consider Disclosure Disclosure to partners is encouraged Pregnancy is key window for disclosure A woman is more likely to disclose during pregnancy, but if she doesn’t disclose then she is likely to do so post-partum 46 Women for Positive Action is supported by a grant from Abbott
Case study 2: HIV+ migrant mother responding to child's diagnosis • HIV+ migrant mother on stable treatment • One older HIV+ son and one younger HIV- daughter who was born in the new home country • Parents both devastated–some of the father’s anger regarding son’s status as been directed at the mother • The mother feels ‘numb’, self-harms and has violent nightmares • She explains ‘I just want to see if I can feel anything. If I can feel pain, I will know I am real’ What support, further questioning, and information can be given? 47 Women for Positive Action is supported by a grant from Abbott
Issues to consider Posttraumatic stress disorder HIV positive women can suffer from PTSD stemming from sexual violence and physical abuse PTSD and depression can often co-occur This disorder is associated with poorer medication adherence and HIV risk behaviour Trauma Trauma history is elevated among HIV-positive women Trauma and abuse are linked with poor medication adherence, HIV risk behaviour and higher levels of emotional illness 48 Women for Positive Action is supported by a grant from Abbott
Conclusions • Stigma of mental illness combined with a HIV diagnosis may lead to compound stress • Burden of emotional disturbance in HIV-positive women is generally under recognised and under treated • Limited access to psychiatric support exists for many HIV-positive women • Medication adherence is affected by mental illness and emotional wellbeing • Introduction of guidelines supporting minimum standards of care is essential Women for Positive Action is supported by a grant from Abbott
Conclusions • Community and peer support can be highly effective • Monitoring the evolving burden of grief, loss and change that emerges as the HIV infection unfolds within a family is important • Use of less stigmatised terminology, such as ‘emotional wellbeing’ may encourage open discussion with those affected by issues relating to: • HIV • Emotional disturbances • Mood disorders Women for Positive Action is supported by a grant from Abbott