Download
1 / 37
380 likes | 803 Views
Elimination of Leprosy. Dr. C.R.Revankar MD, DPH Public Health Physician & Leprologist. Contact :. 3-15-14, Garden view Society, Bhavani Nagar, Marol, Andheri-East, Mumbai(Bombay) - 400059, India Email: macnir@bom3.vsnl.net.in & macnir@juno.com. Leprosy : How important for you.

E N D
Elimination of Leprosy Dr. C.R.Revankar MD, DPH Public Health Physician & Leprologist
Contact : 3-15-14, Garden view Society, Bhavani Nagar, Marol, Andheri-East, Mumbai(Bombay) - 400059, IndiaEmail: macnir@bom3.vsnl.net.in& macnir@juno.com
Leprosy : Howimportant for you Leprosy(Hansen): Easy to diagnose, treat and cure. 3 million people are with leprosy related disabilities in the world.0.76 million new cases were identified in 2001(WHO 2002)
Objectives After this lecture one should be able to- Describe epidemiology of leprosy disease including disability in terms of time trends, impact of leprosy elimination strategies etc
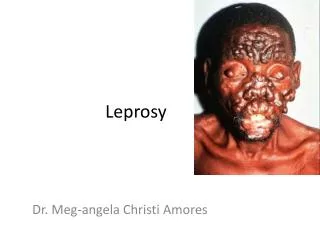
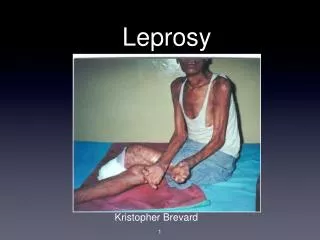
Leprosy (Hansen’s) Disease Chronic infectious disease caused by Mycobacterium leprae, affects nerves, skin and mucosa Causes nerve damage & disabilities - leading to social stigma, ostracism & denial of human rights
Leprosy Case A patient with active signs of leprosy- need or is under MultiDrugTherapy (WHO 1988) Patients with residual signs are Inactive and Cured & should not be included for prevalence rate
Leprosy Elimination Leprosy Elimination:Reducing Prevalence Rate (PR) to less than one active leprosy case per 10,000 population as a Public Health problem (WHO1991) Priority:Communicable part of the disease (Transmission)
Leprosy Eradication/Extinction Eradication: Absence of disease agent in nature in a geographic area after deliberate control measures (WHO2002) Extinction: Specific disease agent no longer exists in nature or laboratory(WHO 2002)
A World Without Leprosy Concept encompasses - early diagnosis, treatment, physical, socio-economic, psychological and rehabilitation of leprosy patients No problems related to Leprosy in the world (ILA 1998)
Global public health strategy-1 • To achieve leprosy elimination • Adequate, regular MDT • Leprosy awareness • Leprosy Elimination campaign • Special Action Projects for • difficult areas (SAPEL)
Global public health strategy-2 • Action plan, review meetings • Resource mobilization, technical • support, Capacity building, drug • supply, monitoring, evaluation & • documentation
Transmission Organism: Mycobacterium leprae Source: Untreated infectious patients (Multibacillary type) Exit: Nasal mucosa, ulcerated skin Entry: Airborne like TB
Epidemiology-1 • 1%-2% exposed population • develop clinical disease • Incubation period: 3-5 years, • can occur after several years • Male:Female ratio: Generally2:1
Epidemiology-2 Geographic variation Lepromatous (MB type) -18% (Tanzania) to 63% (West Malaysia) Neuritic leprosy-18% in India Lucio type - Mexico
Epidemiology-3 • Deformities - 80% in Taiwan • 7.6% in Cameroon • Higher rate of Foot drop in • India and wrist drop in Japan • Prevalence rate—varies from • 10-2500 per 10000 population
Epidemiology-4 Prevalence rate/10000 Agewise 1-5 5-14 >14 (slums) 47 150 247 slums non-slums schools 119 52 66
Global Leprosy Situation-2001 No.of cases registered: 635404Prevalence rate: 1.4 /10000New cases detected: 763317Detection rate: 11.9/100 000South-East Asia region contributed 76.9% of the global case load
Leprosy: top 6 countries-2001 700000 600000 500000 400000 300000 200000 100000 0 India Brazil Nepal Myanmar Madgas'r Moza'que Prevalen Detection
Leprosy: 6 top countries • 6 top endemic countries: India, Brazil, Myanmar, Madgascar, Mozambique, Nepal contribute • 85% of global case load: • (69% from India)• 91% of global case new cases (81% from India)
Magnitude of Disabilities (1995) 1000000 500000 0 B'desh China India Indonesia Thailand Vietnam Guinea Nigeria
Diagnosis of Leprosy More than 95% of cases can be diagnosed clinically even by paramedical workers Skin smears for M.leprae would assist in suspected infectious cases Biopsy/PCR may be needed rarely
Diagnosis- infectious leprosy Detection of 5%-10% skin smear positive leprosy patients is more important as they infect others. If no smear facility, detect 30%-40% of cases with multiple skin lesions.
Paucibacillary leprosy(PBL) From “Leprosy” book by Yawalkar 2002
Multibacillary leprosy(MBL) From “Leprosy” book by Yawalkar 2002
Classification for Treatment • Multibacillary(MB) leprosy: >5 skin lesions:39%•Paucibacillary(PB) leprosy: 2-5 skin lesions:52% • Single skin lesion PB:9% • (WHO 2002)
Multi Drug Therapy • Kill all viable bacteria & make a patient non infectious • Cure an active leprosy patient quickly from a public health point • Residual signs of inactivity may persist including persister bacilli in the deeper tissues
Impact of MDT Program Cases cured: 12 million (2002)Fall in case load: 12 million (1977) to 0.64 million (2002)Deformities prevented:1-2 million Relapse rate: < 1 /1000(WHO 2002)
Cumulative disabled leprosy cases -32 countries-1985-1997
Urban Leprosy Issues-1 • Leprosy Elimination in urban • areas is challenged by - • Rapid increase in population, migration, slum/shanty towns, density, poor living conditions and violence
Urban Leprosy Issues-2 • Favorable to maintain reservoir of infection and transmission • Difficulty in finding hidden cases, • relapse and treatment completion, • private health care participation
Post-Leprosy Elimination issues-1 • Continued transmission • Early detection of MB case, • relapse, rifampicin resistance • Sub clinical infection, carriers • Eradication model, integration • Uniform MDT for six months
Post-Leprosy Elimination issues-2 • Early detection & treatment of • reactions in 30%-40% of cases • Prevention of nerve damage • Prevention & Care of disabled
Post-Leprosy Elimination issues-3 • Patients dissatisfaction for residual • signs after MDT • Immunoprophylaxis • Chemoprophylaxis • Immunotherapy
Partners in Leprosy Elimination WHO, Nippon Foundation, Novartis, World Bank, Danida, ILEP agencies National Governments &NGOs endemic countries