Download
1 / 20
210 likes | 458 Views
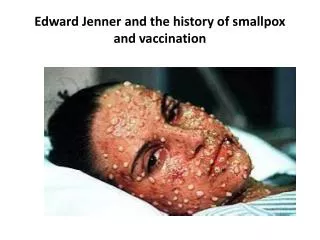
BCG VACCINATION IN THE CONTEXT OF HIV: POLICY AND PRACTICE. Anneke C. Hesseling DEWG Child TB Subgroup 13 October 2009 . BACKGROUND. BCG: Mycobacterium bovis BCG; live, attenuated vaccine given around birth

E N D
BCG VACCINATION IN THE CONTEXT OF HIV: POLICY AND PRACTICE Anneke C. Hesseling DEWG Child TB Subgroup 13 October 2009
BACKGROUND • BCG: Mycobacterium bovis BCG; live, attenuated vaccine given around birth • After polio, most widely given vaccine word-wide: estimated coverage 100.5 million vaccinees in 2002 Multiple BCG strains • Usually given at birth • Marker of EPI vaccine and health program uptake Trunz, Fine, et al. Lancet 2006 Albert Calmette
Global Immunization 1980-2007, BCG coverage at birth global coverage at 89% in 2007 where BCG recommended WHO – EPI, 2008
EFFICACY: BCG IS EFFECTIVE IN PREVENTING SEVERE TB IN CHIDREN • Protection • Consistent60-80% protection against disseminated tuberculosis (TBM, miliary TB) in HIV-negative and unexposed young children • Variable protection: pulmonary TB, limited impact transmission • Revaccination: no benefit • Cost-effective • Limited efficacy data in HIV-infected infants • High TB incidence HIV-infected infants (small subpopulation): 25 fold higher in HIV-infected infants • HAART: reduces risk of TB in HIV-infected infants Trunz, Fine, Dye. The Lancet 2006; 367:1173-1180, Rodrigues, Int J Epi 2002
BCG AND SAFETY • 1. DISSEMINATED BCG DISEASE • Pre-HIV era: incidence 1 -5 per million vaccinees (Fine, 1997) • BCG poses a risk of disseminated BCG disease in infants vertically infected with HIVTalbot et al, Clin Infect Dis 1997, Hesseling, 2003, Hesseling, 2006, Hesseling 2007) • WHO: BCG contra-indicated in individuals with symptomatic HIV infection (2004) • Risk quantification?
REVISED PAEDIATRIC BCG DISEASE CLASSIFICATION Revised paediatric BCG disease classification Local disease Abscess Dual disease M. tb and BCG Regional disease Adenitis BCG IRIS Following HAART Disseminated disease Beyond regional Hesseling et al, Clin Infect Dis 2006
Multi-centre population estimates incidence rates of disseminated BCG disease in HIV-infected children, Western Cape Province, South Africa • Pooled estimate of dBCG incidence: 992 per 100 000 • No HAART, median age 6 months, low CD4 count, mortality >75% • Infant population at risk: 1% Hesseling et al, Bull WHO, 2009
“SAGE agreed that the BCG position paper should be updated to reflect this change and provide guidance to national policy-making bodies, recognizing the complexity of the decision-making process and the lack of information as well as the necessary infrastructure to perform adequate risk assessment in individual children. Among HIV-infected children, the benefits of potentially preventing severe TB are outweighed by the risks associated with the use of BCG vaccine. GACVS therefore advised WHO to change its recommendation such that children who are known to be HIV-infected, even if asymptomatic, should no longer be immunized with BCG vaccine.”
“Since not vaccinating an infant who is exposed to HIV but remains uninfected may increase the risk of disseminated tuberculosis, BCG vaccination should continue in settings where HIV infection and tuberculosis are both highly endemic until it is feasible to implement a policy of selective vaccination. Clear goals should be established for the implementation of safe vaccination practices in HIV-infected infants and for reducing the burden of maternal and infant tuberculosis. More data are needed on the protective effect of BCG vaccination in HIV-infected infants and in HIV-exposed uninfected infants, as well as on the operational feasibility of deferred BCG vaccination In HIV-exposed infants.”
Acute suppurative adenitis 3 weeks after HAART and antituberculosis therapy (BCG IRIS) 2. BCG IRIS
BCG IRIS in infants with baseline CD4≥25%: Early vs. Deferred HAART (CHER study) HAART reduced risk and improves outcome of BCG IRIS – may reduce risk of disseminated BCG? CHER study, Rabie, Cotton et al, CROI, 2008
WHO REVISED POLICY IMPLEMENTATION CONSIDERATIONS IN HIGH-BURDEN SETTTINGS • Quality and access to PMTCT • Infant (maternal) HIV status not known at birth • High risk of M.tb infection • Risk of vertical HIV transmission low - moderate • Capacity for early infant virological diagnosis (PCR) • Access to infant HAART • Ability of EPI and PMTCT programs to implement selective vaccination policy and conduct appropriate follow-up
PROGRAMMATIC CONCERNS • Programmatic confusion regarding selective deferred BCG vaccination of the HIV-exposed infant • Disruption of EPI vaccination program? • Loss of vaccine benefits in HIV-unexposed and in HIV-exposed uninfected infants? • PMTCT programs variable in high-burden settings, HSS • TB screening during pregnancy sub-optimal (HIV); PMTCT programs • Integrated maternal/infant approaches required: PMTCT, TB, child and maternal health, HSS
CONCLUSIONS • BCG is effective in preventing severe childhood TB in the majority of children • BCG is a useful public health intervention in high-burden countries • BCG poses a risk to HIV-infected infants but the magnitude of risk is small in a small subpopulation – risk in context • Guidance: Management of the TB-exposed neonate • Routine programmatic BCG at birth should continue in high-burden settings • Pragmatic guidance being developed for use at program level: WHO EPI, DEWG Child Subgroup
New Diagnostics Working group: Childhood TB subgroup Anneke C. Hesseling and Steve Graham Co-chairs DEWG Childhood TB Subgroup Meeting 12 October 2009
ACTIVITIES YEARS 1 AND 2 • Establishing and maintain a geographically representative membership timeline: high and low-burden countries (n=38; 6% total NDWG) • Launch Official NDWG child subgroup in Cancun with presentation during the NDWG session • Disseminate key information, technical documents, funding, website • Establish links with other ongoing initiatives and subgroups including DEWG Childhood TB Subgroup, TDR, IUATD TREAT-TB • Engagement with WHO Global Plan Update for Research on drugs, diagnostics and vaccine components to include paediatric TB
Map out current paediatric TB diagnostic research activities in the field and promising pilot studies • Develop a scientific "blueprint" for TB diagnostic testing in children: impetus for improved diagnostic testing: improved case finding, testing of new TB vaccines and drug trials rin children • Write NDWG consensus paper editorial on diagnostic challenges and needs in childhood TB • Engage with advocacy groups for diagnostics relevant to children- e.g. TAG, MSF: Cancun meeting 2010 • Linking of diagnostic test strategies into other paediatric TB research platforms (vaccines, trials, contact studies) • Serve as platform for funding of promising pilot studies (seed funding) • Engage with larger research funding agencies