Download
1 / 52
520 likes | 606 Views
Nature of the Immune System. Historical Concepts Specific Immunity Terry Kotrla, MS, MT(ASCP)BB. Age of Serology. Time period from 1900 to 1950 called era of international serology. Immunology is a relatively new science. Tests developed to detect presence of immune substances in the blood.

E N D
Nature of the Immune System Historical Concepts Specific Immunity Terry Kotrla, MS, MT(ASCP)BB
Age of Serology • Time period from 1900 to 1950 called era of international serology. • Immunology is a relatively new science. • Tests developed to detect presence of immune substances in the blood.
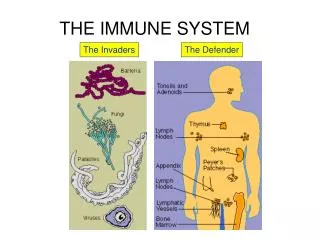
Introduction • Immunology defined as the study of the reaction of a host when foreign substances are introduced into the body. • Immunity is the condition of being resistant to infection. • Serology is the study of the noncellular components in the blood.
Vaccination • Purposeful exposure of individual to infectious material. • Early forms of vaccination were developed in ancient China as early as 200 B.C. • Used powdered scabs from people infected with smallpox was used to protect against the disease.
Vaccination – Edward Jenner • Smallpox affected all levels of society. • Noticed that milkmaids did not generally get smallpox. • Jenner theorized that the pus in the blisters which milkmaids received from cowpox (a disease similar to smallpox, but much less virulent) protected the milkmaids from smallpox.
Vaccination – Edward Jenner • Inoculated 8 yr old with material from pus in cowpox blisters. • Exposed boy to infectious agents and no disease followed. • Jenner's unique contribution was not that he inoculated a few persons with cowpox, but that he then proved they were immune to smallpox.
Vaccination • A vaccine - biological preparation that improves immunity to a particular disease. • A vaccine typically contains a small amount of an agent that resembles a microorganism. • Stimulates the body's immune system to recognize the agent as foreign, destroy it, and "remember" it, so that the immune system can more easily recognize and destroy any of these microorganisms that it later encounters.
Vaccination - Types • Killed microorganisms • Attenuated – live organisms cultivated to disable virulent properties • Toxoid - inactivated toxic compounds in cases where these (rather than the micro-organism itself) cause illness • Subunit -fragment create an immune response • Conjugate-linking outer coats to proteins which can the lead immune system to recognize
Rabies • Louis Pasteur applied this principle of attenuation to a rabies vaccine. • Developed a rabies virus that was milder and had a shorter incubation (development) period than the wild virus. • A person bitten by a rabid animal would be inoculated with the Pasteur virus and rapidly develop immunity to the wild strain.
Rabies • He developed his rabies vaccine by growing the virus in rabbits, then drying the affected nerve tissue to weaken the virus. • On July 6, 1885, the vaccine was administered to a 9-year-old boy who had been attacked by a rabid dog. • The boy survived and avoided contracting rabies, which would have almost certainly proved fatal.
Cellular versus Humoral Immunity • Cellular - Researchers observed that foreign substances were removed by specialized cells in a process known as phagocytosis. • Humoral - Other researchers postulated that substances in the blood provided protection from microorganisms, humoral immunity.
Natural (Nonspecific , Innate) Immunity • Non-specific immunity • First line of defense against infection • Uses body functions • Coughing, sneezing, cilia • HCl in stomach, wax in ears, enzymes in tears • Circulating and tissue cells • Circulating substances • Two mechanisms – external and internal
Physiological factors • Stomach acid kills pathogens and sterilizes food. • Mucus lining of lungs traps pathogens and cilia move particles out to throat and it is swallowed. • Tears wash away pathogens and have bacteriocidal enzymes. • Flushing action of urine • Skin: Difficult for a pathogen to penetrate, sweat creates high salt conditions, oil layer makes an inhospitable environment. • Normal flora prevents growth of opportunistic pathogens in mouth, large intestine and reproductive system
Factors Modify Defense Mechanisms • Age • Hormones • Drugs and chemicals • Malnutrition • Fatigue and stress • Genetic determinants
Nonspecific Immunity: Second line of defense • Inflammatory response - four classic signs are redness, swelling, heat and pain. • Dilation of capillaries (hyperemia) to increase blood flow to area • Chemotaxis - chemicals released which cause phagocytic white cells to migrate to the area. • Increased capillary permeability allowing white cells to go to injured area, a process known as “diapedesis” • Formation of exudate - same composition as plasma and it contains antibacterial substances, phagocytic cells, and drugs and antibiotics, if present.
Second Line of Defense • If bacteria are not successfully killed locally, may further invade the host by way of the lymphatics to the regional lymph nodes. • within lymph nodes the bacteria meet other phagocytic cells • bacteria may overcome these and gain access to the bloodstream where they meet circulating phagocytes (neutrophils and monocytes). • may pass through the bloodstream and reach organs such as the liver and spleen where they come into contact with tissue macrophages. • although a powerful defense system, this final phagocytic barrier may be overcome, with seeding of the microorganism to organs such as bone, brain, and kidney, terminating in fatal septicemia.
Phagocytosis • Initiation is caused by damage to the tissues, either by trauma or as a result of microbial multiplication. • Chemotaxis, attraction of leukocytes or other cells by chemicals. • Opsonization - Opsonization coating a pathogen by substances so as to enhance phagocytosis. • Adherence, firm contact between phagocyte and microorganism. • Engulfment into cytoplasm and enclosed in a vacuole. • Digestion enzymatic contents in vacuole destroy the microorganism. • Number of killing mechanisms operating in the vacuoles of phagocytic cells. • One of the major mechanisms involves hydrogen peroxide which, acting along with an intracellular enzyme, is rapidly lethal to many bacteria.
Phagocytosis • http://www.cellsalive.com/ouch.htm • http://health.howstuffworks.com/adam-200096.htm • http://tinyurl.com/6oa779
Cells of the Non-Specific Immune System • Cells involved in non specific immunity. • Phagocytic cells • Mononuclear phagocytes • Polymorphonuclear phagocytes • Eosinophils • Mediator cells • Basophils and mast cells • Platelets
Cells involved in specific immunity • Lymphocytes • Plasma cells
Origin of immune cells • Origin of all these cell types are stem cellsfound in the bone marrow. • These self replicating cells differentiate into two types of "committed" stem cells. • One group differentiates further and matures to become platelets, erythrocytes (red blood cells), monocytes or granulocytes. • Second group produces cells of the lymphoid lineonly. • The lymphoid line will develop into 2 different types, T and B cells, depending upon where they complete their maturation, thymus or bone marrow.
Phagocytic Cells • Mononuclear phagocytes- include both circulating bloodmonocytes and tissue macrophages found in various tissues of the body. • Arise from bone marrow stem cells • Not end cells, they may divide. • Ingest and destroy material such as bacteria, damaged host cells or tumor cells (non-specific immunity). • Stay in peripheral blood 70 hours - migrate to tissues, double in size, then called tissue macrophages. • Tissue macrophages named according to tissue location- liver=Kupffer cells, brain-microglial cells, etc. • Phagocytosis takes place to a greater degree in tissues.
Polymorphonuclear phagocytes • AKA Neutrophils • Characterized bya large nucleus, usually with 3 - 5 lobes, and the presence of numerous, specific granules in the cytoplasm. • Arise from bone marrow stem cells. • They are end cells. • Primary function is ingestion (phagocytosis). • Clear body of debris such as dead cells and thrombi. • Able to move into tissues by diapedesis -wander randomly
Eosinophils • Easily distinguished by the presence of largegranules in their cytoplasm which appear red when stained by routine hematology stains. • Much less phagocytic than macrophages or neutrophils • Function is far from clear, however the numbers increase greatly in certain parasitic diseases and allergic diseases. • Both neutrophils and eosinophilscontain specific granules, the granules contain various enzymes which are released under certain circumstances.
Mediator Cells • Influence the immune response by releasing various chemical substances into the circulation. • Have a variety of biological functions • Increase vascular permeability • Contract smooth muscle • Enhance the inflammatory response • Two types • basophils/mast cells • Platelets
Basophils and Mast cells • Basophils easily identified due to large numbers of bluish-black granules in the cytoplasm. • The granules are a source of mediators such as histamine (vasoactive amine that contracts smooth muscle) and heparin. • Basophils and platelets are found in the circulation, mast cells are situated in the tissues of skin, lung and GI tract. • Circulating basophils greatly resemble tissue mast cells and it is likely that they are closely related in function. • Both of these cells play a role in hypersensitivity (allergic) reactions.
Platelets • Small non-nucleated cells derived from megakaryocytesof the bone marrow. • Important in blood clotting. • Contribute to the immunological tissue injury occurring in certain types of hypersensitivity reactions by releasing histamineand related substances which are contained within specialized granules in their cytoplasm.
Soluble Factors • Many soluble tissue and serum substances help to suppress the grow of or kill microorganisms. • Interferons - family of proteins which are important non-specific defense mechanisms against viral infections. • Transferrin - Bacteria do not thrive well in serum that contains low levels of iron but high levels of transferrin. • Complement - a group of proteins that are essential for bacterial destruction and plays an important role in both non-specific and specific immune mechanisms.
Acute Phase Proteins • Defined-normal serum constituents that increase rapidly because of infection, injury, or trauma to tissues. • Acute-phase proteins are a class of proteins whose plasma concentrations increase or decrease in response to inflammation. • This response is called the acute-phase reaction . • In response to injury local inflammatory cells (neutrophils, granulocytes and macrophages) secrete a number of cytokines into the bloodstream, most notable of which are the interleukins. • The liver responds by producing a large number of acute-phase reactants.
C-Reactive Protein • Increases rapidly within 4-6 hours of infection or injury. • Returns to normal rapidly once condition subsides. • Used to monitor healing and has also increased in usefulness in diagnosing Myocardial Infarction.
Complement • A series of serum proteins involved in mediation of inflammation but also involved in • opsonization, • chemotaxis, and • cell lysis.
Alpha-1 Antitrypsin • Plays important role preventing breakdown of enzymes in various organs of the body and protects the lungs so they can work normally. • When the lungs do not have enough alpha-1 antitrypsin, neutrophil elastase is free to destroy lung tissue. • As a result, the lungs lose some of their ability to expand and contract (elasticity). This leads to emphysema and sometimes makes breathing difficult.
Haptoglobin • Binds irreversibly to free hemoglobin to protect kidneys from damage and prevent loss of iron by urinary excretion. • Haptoglobin - hemoglobin complex removed by RES, mainly spleen. • Used to monitor hemolysis
Fibrinogen • A coagulation factor integral to clot formation which serves as a barrier to prevent spread of microorganisms further in the body. • Levels increase with tissue inflammation or tissue destruction. • Thought to play a key role in the inflammatory response and development of rheumatoid arthritis.
Ceruloplasmin • The major copper containing protein in plasma, plays a role in iron metabolism and histamine regulation. • Stimulates the immune system to fight infections, repair injured tissues and promote healing. • Depletion found in Wilson’s disease, causes the body to absorb and retain excessive amounts of copper. • Copper deposits in the liver, brain, kidneys, and the eyes. • The deposits of copper cause tissue damage, necrosis (death of the tissues), and scarring, which causes decreased functioning of the organs affected. • Liver failure and damage to the central nervous system (brain, spinal cord) are the most predominant, and the most dangerous, effects of the disorder.
Alpha-1 Acid Glycoprotein(AGP) • An acute phase protein manufactured in the liver and found in the blood of humans and animals. • In simplest form, detection of elevated levels of AGP has been shown to indicate background illness or other stressors when animals appear clinically normal. • Acute phase proteins such as AGP are elevated during acute or chronic periods of inflammation or infectious diseases, following surgery, with malignant tumors, in autoimmune diseases, liver cirrhoses and with all types of stress in general. • Other effects related to elevated levels of AGP are immunosuppression, poor response to vaccines, etc.