Download
1 / 9

E N D
Case History • CC: Left leg pain. • HPI: 15 yo female reports feeling a “snap” in her left leg while running sprints at volleyball practice. She felt immediate pain with inability to bear weight. Patient presented to ER for evaluation. She denies any trauma to her leg or similar incidents in the past. Denies loss of consciousness, chills, fever, SOB, chest pain, N/V. • PMH: Asthma, Occasional temporal/frontal HA • No significant PSurHx, Social Hx. NKDA. • Medications: Ortho Tri-Cyclen
H&P Continued • Vitals: T: 36.5 BP: 105/59 P: 71 R: 20 O2: 100% • PE: Patient NAD, AAOX3. Pt. able to move all aspects of LLE but not w/o extreme pain. 2+ dorsalis pedis and posterior tibial pulses. Sensation intact. • Plain films of LLE taken. 2 views ordered: Pelvis, single view w/ left hip; Left femur, single view. • In ER, pt. LLE put in 20 lbs traction after insertion of traction pin on proximal left tibia.
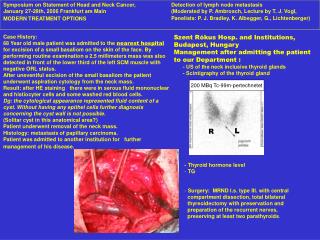
Findings • Impression of plain films: • Cystic expanding lesions w/in left femoral neck and proximal shaft of left femur, most likely consistent with fibrous dysplasia. • Pathologic fracture of proximal left femur. • DDX of cystic expanding lesions in bone: • Fibrous dysplasia • Enchondroma • Small bones, typical calcifications in rings or arc pattern • Unicameral bone cyst • Fluid filled cyst • Aneurismal bone cyst • Commonly in spine, assoc. w/ trauma, “soap bubble” appearance • Giant cell tumor • 3rd decade, closed epiphyseal plates, central lucency, peripheral density • Low Grade Osteosarcoma • “Cloudlike” appearance, involves soft tissue, cortical discontinuity
Fibrous Dysplasia • Skeletal development anomaly in which medullary bone is replaced by fibrous tissue. Presents with bone pain, limp, limb-length discrepancy, or pathologic fracture. • Ages 3-15 yo; M=F; 5-7% of benign bone tumors. • Monostotic (70%) vs. Polystotic (30%) • Polystotic associated with McCune Albright Syndrome, Cushing syndrome, hyperthyroidism, and hyperparathyroidism. • Treatment options: Bisphosphonates; Surgery; Observation • Plain radiograph is first line study: • Relatively homogenous cyst with characteristic ground-glass or “smokey” appearance. • Absent periosteal reaction. • May have then sclerotic rim around cyst with cortical thinning. • “Shepherd’s crook” deformity of proximal femur
Hospital Course • Patient was taken to OR for intramedullary nail of her left femur with 26x11.5 titanium Recon nail. • During procedure, pathologic specimens of bone cyst were obtained and sent to pathology. • POD #1: patient w/ decreased swelling and increased LLE motion. • POD #2: patient ambulating w/ crutches per PT evaluation. Patient discharged home with pain medications.
References • Favus MJ, Vokes T. Harrison’s Principles of Internal Medicine, 16th Ed. Section 2. 2005. • DiCaprio MR, Enneking WF. “Fibrous Dysplasia: Pathophysiology, Evaluation, and Treatment.” The Journal of Bone and Joint Surgery. 2005; 87: 1848-1864. Presentation by: Amee Patel 4th Year Visiting Student Georgetown University