Download
1 / 48
490 likes | 974 Views
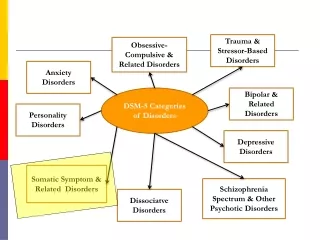
Treatment of Schizophrenia (and Related Psychotic Disorders). Scott Stroup, MD, MPH 2007. Psychosis. Generally equated with positive symptoms and disorganized or bizarre speech/behavior Impaired “reality testing” A syndrome present in many illnesses

E N D
Treatment of Schizophrenia (and Related Psychotic Disorders) Scott Stroup, MD, MPH 2007
Psychosis • Generally equated with positive symptoms and disorganized or bizarre speech/behavior • Impaired “reality testing” • A syndrome present in many illnesses • remove known cause or treat underlying illness • treat symptomatically with antipsychotic medications
Schizophrenia is a heterogeneous illness • Defined by a constellation of symptoms, including psychosis • Multifactorial etiology, variable course • Social/occupational dysfunction a required diagnostic criterion • Good treatment must address symptoms and social/occupational dysfunction
Features of Schizophrenia Positive symptomsDelusionsHallucinations Disorganization Speech Behavior Functional ImpairmentsWork/schoolInterpersonal relationshipsSelf-care Cognitive deficitsAttentionMemory Verbal fluencyExecutive function (e.g., abstraction) Mood symptomsDepression/AnxietyAggression/Hostility Suicidality Negative symptomsAnhedonia Affective flatteningAvolitionSocial withdrawal Alogia Negative symptoms may be due to primary “deficit pathology” or secondary to positive symptoms and/or drug side effects
Challenges in the Treatment of Schizophrenia • Stigma • Impaired “insight”– no agreement on problem • Treatment “compliance” • Substance abuse very common • Violence risk • Suicide risk • Medical problems common, often unrecognized
Schizophrenia Treatment • Therapeutic Goals • minimize symptoms • minimize medication side effects • prevent relapse • maximize function • “recovery” • Types of Treatment • pharmacotherapy • psychosocial/psychotherapeutic
Treatments for schizophrenia:Strong evidence for effectiveness • Antipsychotic medications • Family psychoeducation • Assertive Community Treatment (ACT teams)
The First Modern AntipsychoticChlorpromazine (Thorazine) • Antipsychotic properties discovered in 1952 • Studied originally for usefulness as a sedative • Found to be useful in controlling agitation in patients with schizophrenia • Introduced in U.S. in 1953
Show Video Tape Augustine
The Dopamine Hypothesis of Schizophrenia • All antipsychotics block the dopamine D2 receptor • Conventional antipsychotic potency is directly proportional to dopamine receptor binding • Dopamine enhancing drugs can induce psychosis (e.g., chronic amphetamine use)
Somatic Treatments for Psychotic Disorders 30s ‘40s ‘50s ‘60s ‘70s ‘80s ‘90s ‘00 ECT Reserpine Haloperidol Fluphenazine Thioridazine Loxapine Perphenazine Clozapine Lobotomy Risperidone Olanzapine Quetiapine Ziprasidone Aripiprazole Chlorpromazine Paliperidone First Generation Antipsychotics Second Generation Antipsychotics
“Typical” antipsychotic medications(aka first-generation, conventional, neuroleptics, major tranquilizers) • Low Potency (300-800+ mg/day)(chlorpromazine, thioridizine) • Mid Potency (loxapine, perphenazine) • High Potency (2-20 mg/day)(haloperidol, fluphenazine)
Dopamine blockade effects • Limbic and frontal cortical regions: antipsychotic effect • Basal ganglia: Extrapyramidal side effects (EPS) • Hypothalamic-pituitary axis: hyperprolactinemia
Antipsychotic limitation: Extrapyramidal side effects (EPS) • Parkinsonism • Akathisia • Tardive dyskinesia (TD)-- the worst form of EPS-- involuntary movements • These have historically been associated mostly, but not exclusively, with conventional antipsychotics
Parkinsonian side effects • Rigidity, tremor, bradykinesia • Management: • Lower antipsychotic dose if feasible • Change to different drug (i.e., to an atypical antipsychotic) • Anticholinergic medicines: • benztropine (Cogentin) • trihexylphenidine (Artane)
Akathisia • Restlessness, pacing, fidgeting; subjective jitteriness; associated with suicide • Resembles psychotic agitation, agitated depression • Management: • Lower antipsychotic dose if feasible • Change to different drug (i.e., some atypical antipsychotics) • Adjunctive medicines: • propanolol (or another beta-blocker) • benztropine (Cogentin) • benzodiazepines
Show Tardive Dyskinesia Videotape Abnormal Involuntary Movement Scale (AIMS) training tape
Tardive Dyskinesia (TD) • Involuntary movements, often choreoathetoid • Often begins with tongue or digits, progresses to face, limbs, trunk • Etiologic mechanism unclear (dopamine receptor supersensitivity?) • Incidence about 3% per year with typical antipsychotics • Higher incidence in elderly
Tardive Dyskinesia (TD)-2 • Major risk factors: • high doses, long duration, increased age, women, history of Parkinsonian side effects • Prevention: • minimum effective dose, atypical meds, monitor with AIMS test • Treatment: • lower dose, switch to atypical, Vitamin E (?)
Antipsychotic limitation: Other common side effects • Anticholinergic side effects: dry mouth, constipation, blurry vision, tachycardia • Orthostatic hypotension (adrenergic) • Sedation (antihistamine effect) • Weight gain • “Neuroleptic dysphoria”
Antipsychotic limitation: Refractory Symptoms • Poor treatment response in 30% of patients • Incomplete treatment response in an additional 30% or more
The First “Atypical” Antipsychotic:Clozapine (Clozaril) • FDA approved 1990 • For treatment-resistant schizophrenia • 30% response rate in severely ill, treatment-resistant patients (vs. 4% with chlorpromazine/Thorazine) • Receptor differences: Less D2 affinity, more 5-HT 10
Clozapine: pros and cons • Superior efficacy for positive symptoms • Possible advantages for negative symptoms • Virtually no EPS or TD • Advantages in reducing hostility, suicidality • Associated with agranulocytosis (1-2%) • WBC count monitoring required • Seizure risk (3-5%) • Warning for myocarditis • Significant weight gain, sedation, orthostasis, tachycardia, sialorrhea, constipation • Costly—but generic now available • Fair acceptability by patients and doctors
Defining “atypical” antipsychotic(aka second-generation, novel) Relative to conventional drugs: • Lower ratio of D2 and 5-HT2A receptor antagonism • Lower propensity to cause EPS (extrapyramidal side effects)
Atypical Antipsychotics: Efficacy • Effective for positive symptoms • (similar to typical antipsychotics) • Only clozapine has been consistently more effective than conventional antipsychotics in patients with refractory psychotic symptoms • Atypicals may be better than conventionals for negative symptoms—if so, this is likely because they cause fewer negative symptoms due to EPS than conventionals at doses used in most available studies
Atypical Antipsychotics: Efficacy for Cognitive and Mood Symptoms • Atypical antipsychotics may improve cognitive symptoms • Dysphoric mood may be more common with typical antipsychotics
Atypical Antipsychotics: Side Effects • Atypical antipsychotics tend to have better subjective tolerability (except clozapine) • Atypical antipsychotics are thought to be less likely to cause EPS and TD, but may cause more: • Weight gain • Metabolic problems (lipids, glucose)
Weight gain at 10 weeks Kg Allison et al 1999
Summary of Antipsychotic Side Effects Side Effect Highest Liability Low Liability EPS High-potency conventional CLZ, OLZ, QTP antipsychotics TD Conventional CLZ, OLZ, QTP antipsychotics Hyperprolactinemia Conventional CLZ, OLZ, QTP antipsychotics, RIS Sedation CPZ, CLZ, QTP, OLZ RIS Anticholinergic CPZ, CLZ, QTP RIS effects QTc prolongation thioridazine, mesoridazine, ZIP Weight gain CPZ, CLZ, OLZ HAL, ZIP Hyperglycemia, DM Atypical antipsychotics
2004 clinical consensus on antipsychotics • Atypical antipsychotics (other than clozapine) are first choice drugs:-superiority on EPS and TD-at least equal efficacy on + and – symptoms-possible advantages on mood and cognition • BUT:-long-term consequences of weight gain and metabolic effects may alter recommendation-atypicals are very expensive
State of the Evidence: Key Recommendations of the Schizophrenia Patient Outcomes Research Team (PORT) • No clear statement of preference of SGAs over FGAs in acute or maintenance treatment • Clozapine is the treatment of choice for treatment-refractory positive symptoms; also recommended for hostility and suicidality • Long-acting antipsychotics recommended for individuals who do not adhere to oral medication regimens Lehman AF, et al. Schizophrenia Bulletin. 2004
Antipsychotic prescriptions in U.S. TRx (000s) Source: Verispan PDDA; IMS NPA Plus, March 2006
CATIE Phase 1: Double-blinded and randomized Olanzapine 7.5-30 mg/day Perphenazine 8-32 mg/day 1460 participants with schizophrenia Quetiapine 200-800 mg/day Risperidone 1.5-6 mg/day Ziprasidone 40-160 mg/day Randomized Participants followed for 18 months
Time to Discontinuation for Any Reason Overall p-value = 0.004* P<0.001 for olanzapine vs quetiapine P=0.002 for olanzapine vs risperidone
Summary of CATIE findings • Overall, all the drugs similar • One drug, olanzapine, was somewhat more effective than the others but caused more weight gain and metabolic problems • The older drug, perphenazine, did not cause more EPS than the other drugs; it was just as effective as 3 of the drugs; it costs much, much less than the newer drugs • No advantage of the newer drugs on negative symptoms • No advantage of the newer drugs on cognitive functioning • Perphenazine most cost effective • Issue of Tardive Dyskinesia not answered
Common factors associated with psychotic relapse • antipsychotics not completely effective • “noncompliance”—inconsistent antipsychotic medication use • stressful life events/home environment • alcohol use • drug use
Consequences of relapse • Disruptive to patients lives(hospitalizations, lost jobs, lost apartments, estranged family and friends) • Risk of dangerous behaviors • May worsen course of illness • Increased costs
Antipsychotic medication reduces relapse rates Risk of relapse in one year: Consistently taking medications: 20-30% Not taking medications consistently: 65-80%
Long-acting injectable (depot) antipsychotics • Goal is to decrease “noncompliance” and thus relapse--widely used but less commonly in last 10 years • Injections every 2 weeks (fluphenazine and risperidone) or 4 weeks (haloperidol) • Not yet clear if long-acting risperidone will reverse the trend of decreased depot use
Drug Treatments for Features of Schizophrenia Positive symptomsDelusionsHallucinations Antipsychotic drugs Disorganization Speech Behavior Antipsychotic drugs Functional ImpairmentsWork/schoolInterpersonal relationshipsSelf-care Cognitive deficitsAttentionMemory Verbal fluencyExecutive function (e.g., abstraction) No proven drug treatments Mood symptomsDepression/AnxietyAggression/Hostility Suicidality Choices include: Antidepressants, mood stabilizers, and antipsychotics (especially clozapine) Negative symptomsAnhedonia Affective flatteningAvolitionSocial withdrawal Alogia Primary (deficit pathology)-----No proven drug treatments Secondary to extrapyramidal side effects (EPS)-----Minimize EPS with dose and drug selection; Treat EPS Secondary to positive symptoms-----Antipsychotic drugs
Schizophrenia TreatmentAssertive Community Treatment • Multidisciplinary teams: MDs, RNs, social workers, psychologists, occupational therapists, case managers • Staff:patient ratio about 1:10 • Outreach, contact as needed • Effective at reducing hospitalizations • Cost-effective when targeted at high hospital users
Schizophrenia TreatmentFamily Psychoeducation • Provides information about schizophrenia: course, symptoms, treatments, coping strategies • Supportive • Not blaming
Schizophrenia TreatmentPsychotherapy (individual or group) • Supportive • Cognitive-behavioral • “Compliance” therapy • Psychoeducational • Not regressive / psychoanalytic
“Deinstitutionalization” • Mid-1950s: >500,000 people in state psychiatric hospitals • Now: <<100,000 • Antipsychotic medications • Civil (patients) rights movement • Community Mental Health Acts (1963-64) • Medicaid (1965-allows states to share costs with federal government) • Still an active issue in N.C.—adequacy of community-based services remain in doubt
Recommended books on schizophrenia • Is there no place on earth for me?, Susan Sheehan • Imagining Robert,Jay Neugeboren • Nightmare: a schizophrenia narrative, Wendell Williamson • The Quiet Room, Lori Schiller