Download
1 / 40
400 likes | 502 Views
Understand pleural anatomy, pathophysiology of effusions, diagnostic techniques like thoracentesis, Light's criteria, and differential diagnosis of transudates vs exudates in managing pleural effusions effectively.

E N D
Clinical Approach to PLEURAL EFFUSIONS
PLEURAL SPACE The pleura consists of 2 layers 1 – parietal pleura 2 – visceral pleura The space between the 2 layers is called the pleural space Normal width of the pleural space is 10-20 mm
Pleura Visceral pleura envelope all surfaces of the lungs, including the interlobar fissures. Parietal pleura cover the inner surface of the thoracic cavity, including the diaphragm, and ribs. At the Hilum where pulmonary vessels, bronchi, and nerves enter the lung tissue, the parietal pleura is continuous with the visceral pleura.
PLEURAL EFFUSION • Normally the pleural space contains: • 3.5 to 7.0 ml of clear liquid • low protein content • small number of mononuclear cells • Pleural effusion: presence of large amount of fluid in the pleural space irrespective of the underlying causes
PLEURAL FLUID FORMATION AND ABSORTION PLEURAL SPACE INTERCOSTAL MICROVESSELS BRONCHIAL MICROVESSELS VEIN VEIN ARTERY ARTERY ? LYMPHATICS TO MEDIASTINAL NODES PLEURAL FLUID STOMA PLEURAL SPACE PARIETAL PLEURAL VISCERAL PLEURAL
MOVEMENTS OF FLUID IS BASED ON STARLING’S LOW STARLING’S LOW : L . A [ (PCAP– PPl) – (CAP–Pl) ] L: Filtration coefficient A: Surface area Cap: Capillary Pl: Pleural
PLEURAL FLUID FORMATION AND ABSORTION • The rate of fluid formation is 0.02 ml/kg/hour. • The rate of fluid clearance is 0.2 ml/kg/hour.
PLEURAL FLUID FORMATION AND ABSORTION PLEURAL SPACE INTERCOSTAL MICROVESSELS BRONCHIAL MICROVESSELS VEIN VEIN ARTERY ARTERY ? LYMPHATICS TO MEDIASTINAL NODES PLEURAL FLUID STOMA PLEURAL SPACE PARIETAL PLEURAL VISCERAL PLEURAL
Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) plasma oncotic pressure (hypoalbuminemia) pleural membrane permeability (malignancy) lymphatic obstruction (malignancy) diaphragmatic defect (hepatic hydrothorax) thoracic duct rupture (chylothorax)
Symptoms * key symptom -------> shortness of breath Fluid filling the pleural space makes it hard for the lungs to fully expand, causing the patient to take many breaths so as to get enough oxygen. * If parietal pleura is irritated ------->mild painor a sharp stabbing pleuritic type of pain. ** Some patients will have a dry cough.
Symptoms Occasionally ------> no symptoms at all. * This is more likely when the effusion results from: recent abdominal surgery, cancer, or tuberculosis. * Tapping on the chest will show stony dullness, and decrease breath sound
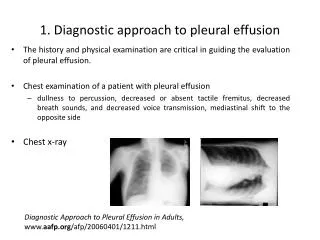
Diagosisn of pleural effustion • x ray • The fluid itself can be seen at the bottom of the lung or lungs, hiding the normal lung structure. • If heart failure is present, • the x-ray shadow of the heart will be enlarged. Ultrasound may disclose a small effusion that caused no abnormal findings during chest examination. C.T. scan is very helpful if the lungs themselves are diseased.
PLEURAL EFFUSION Indication for Pleural Fluid Analysis • Diagnostic ( detect underlying diagnosis) • Therapeutic (relief shortness of breath)
PLEURAL EFFUSION DIAGNOSTIC THORACENTESIS • CONTRAINDICATIONS • Bleeding tendency • Thrombocytopenia (decrease platelets less 25000 u3/dl ) • Prolonged PT or PTT greater than twice normal, • A very small volume of pleural fluid
Color of Fluid Color of Fluid Suggested Diagnosis Pale yellow (straw) Transudate, some exudates Red (bloody) Malignancy or embolism or TB Turbid Infected effusion PusEmpyema White (milky) Chylothorax or cholesterol effusion
Transudates vs Exudates LIGHT’S CRITERIA* 1. Pleural Protein divided by serum protein >0.5 2. Pleural fluid LDH divided by Serum LDH >0.6 3. Pleural fluid LDH > 2/3 the upper limit of normal for the serum LDH.
Causes of Transudates and Exudates Tronsudote Exudate Left Heart Failure Bacterial Pneumonia Hypoproteinaemia Carcinoma Bronchus Constrictive Pericarditis Pulmonary Infarction Hypothyroidism Tuberculosis Connective-tissue Disease Cirrhosis
PLEURAL EFFUSION • CELL COUNT • Transudate < 1000 but 20% > 1000 and rarely > 10,000/mm3 • Exudate > 1000/mm3 • Limited value (unless > 50,000/mm3 emphyema)
PLEURAL EFFUSION PF LYMPHOCYTE-PREDOMINANT EXUDATES (>80%) Causes TB Lymphoma `Chronic lymphocytic leukaemia
PLEURAL EFFUSION BIOCHEMISTY Glucose < 3.3 mmol/L or 1/2 serum glucose (simultaneous) - Rheumatoid pleurisy (85%) - Empyema (80%) - Malignancy (40%)
PLEURAL EFFUSION The mechanism responsible for pleural fluid low glucose include; • Decreased transport of glucose from blood to pleural fluid • Increased utilization of glucose by constituents of pleural fluid, such as neutrophils, bacteria (empyema), and malignant cells
PLEURAL EFFUSION • BIOCHEMISTY • Pleural fluid pH: • - Normal pleural fluid pH is > 7.6 • - Transudates – pH 7.40-7.55 • - Exudates – pH is 7.30-7.45 • Should always be measured in a blood gas machine • Parapneumonic - pH < 7.0 predicts “complicated effusion” that is unlikely to resolve without chest tube drainage. • Malignant effusion with a pH < 7.3 is associated with poor survival. • If pH < 6.0 think of ruptured esophagus
PLEURAL EFFUSION The mechanism responsible for pleural fluid acidosis (pH <7.30) include; • Increased acid production by pleural fluid cells and bacteria • Decreased hydrogen ion efflux from the pleural space, due to pleuritis, tumor, or pleural fibrosis.
PLEURAL EFFUSION DIAGNOSES ASSOCIATED WITH PLEURAL FLUID ACIDOSIS (pH <7.30) AND LOW GLUCOSE CONCENTRATION (PF/SERUM <0.5) Diagnosis Usual pH (Incidence) Usual Glucose Concentration (mg/dL) Empyema 5.50-7.29 (-100%) <40 Malignancy 6.95-7.29 (33%) 30-59 Tuberculous pleurisy 7.00-7.29 (20%) 30-59
PLEURAL EFFUSION • CYTOLOGY • positive in about 60% of patients with malignant effusion
PLEURAL EFFUSION Patients with Abnormal Chest Radiograph Suspect pleural disease Blunting of costophrenic angle? YES Lateral decubitus chest radiographs Yes No Diagnostic thoracentesis Fluid thickness > 10mm Observe
PLEURAL EFFUSION SUMMARY Diagnostic thoracentesis Any of the following met? PF/serum protein >0.5 PF/serum LDH >0.6 PF LDH >2/3 upper normal Serum limit Yes No Exudate Transudate Appearance of plueral fluid, pH & glucose, cytology and differential cell count of pleural fluid Treat CHF, cirrhosis, or nephrosis
Best Way Treatment direct treatment at what is causing it, rather than treating the effusion itself
pneumothorax • Peneumothorax is the accumulation of air in the pleural space. It may occur spontaneously or following trauma Disorder Cause Collection Chest trauma; rupture of aortic aneurysm Haemothorax Blood Congestive cardiac failure Hydrothorax Proteinaceous Fluid Chylothorax Lymph Neoplastic infiltration; trauma Pneumothorax Air Spontaneous; traumatic
Spontaneous Results from rupture of a pleural bleb Pleural bleb being a congenital defect of the alveolar wall connective tissue. Patients are typically tall, thin, young males. M:F ratio 6:1. Usually apical affecting both lungs with equal frequency.
Spontaneous Secondary causes occur in patients with underlying disease : COPD, TB, pneumonia, bronchial carcinoma, sarcoidosis and cystic fibrosis.
Spontaneous Patients present with sudden onset of unilateral pleuritic pain and increasing breathlessness. The main aim of treatment is to get the patient back to active life as soon as possible.
Investigations Chest radiography may show an area devoid of lung markings. May be more clearly seen on the expiratory film
Management Small pneumothorax: no treatment, but review in 7-10 days. Moderate pneumothorax: admit for simple aspiration.