Download
1 / 13
130 likes | 266 Views
Human Cytomegalovirus (HCMV) Proposed 1 st International Standard WHO/BS/08.2099 Jacqueline Fryer. Rationale 1. Ubiquitous and persistent infection, causes disease in immunologically naïve (foetus and newborns) and suppressed (transplant recipients, AIDS patients).

E N D
Human Cytomegalovirus (HCMV) Proposed 1st International StandardWHO/BS/08.2099Jacqueline Fryer
Rationale 1 • Ubiquitous and persistent infection, causes disease in immunologically naïve (foetus and newborns) and suppressed (transplant recipients, AIDS patients). • Leading infectious cause of deafness and brain damage in newborns, most significant viral pathogen after solid-organ transplantation. • High viral load is most important risk factor for CMV disease in transplant recipients; HCMV DNA quantification assays are used to guide pre-emptive antiviral therapy to prevent viral load rising above critical disease threshold. • Viral load measurements increasingly being used to predict sensorineural hearing loss congenitally-infected infants.
Rationale 2 • Viral load measurements performed using NAT, particularly real-time PCR. Many assays developed in-house, although a number of new commercial assays have been developed. • High level of inter-laboratory variability in viral load measurements (AST/CST study, EQA proficiency programmes). • Cut-off thresholds for initiation of pre-emptive therapy are site-specific and vary significantly, therefore, difficult to compare clinical practice and standardise patient management. • IHMF* recommendations (2004) called for ‘international quantification standard to compare studies using different PCR-based systems and facilitate patient management at multiple care centres’. * International Herpes Management Forum
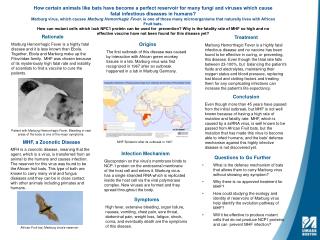
Rationale 3 Variability in performance of HCMV viral load assays Plasma spiked with HCMV Merlin Clinical samples Log10 variation in reported results (relative to expected) Pang et al, Am J Transplant. 2009;9:258-68
Source material for HCMV candidate • Whole virus preparation of prototype clinical HCMV strain Merlin • Produced in cell culture, formulated in universal buffer and freeze dried • Concentration of ~1x107 copies/mL (IU when established) • ~5000 vials to be filled (August 2009)
Collaborative study protocol • Candidate standard to be evaluated alongside frozen liquid preparations: • Merlin liquid bulk • Prototype laboratory HCMV strain AD169 (whole virus) • Purified BAC-cloned Merlin DNA • ~30 participants (clinical and research labs, assay manufacturers) performing range of NAT-based assays • To ECBS 2010
Intended use • Calibration of secondary references used in routine HCMV viral load assays • Calibration/validation of commercial NAT assays • Evaluation of HCMV-positive materials distributed in molecular quality assurance programmes
Epstein-Barr Virus (EBV) Proposed 1st International StandardWHO/BS/08.2099
Rationale 1 • EBV-associated Post Transplant Lymphoproliferative Disease (PTLD) affects 1-20% of allografts. • Viral load measurements by NAT used to guide pre-emptive therapy in transplant recipients. • High level of inter-laboratory variability in viral load measurements (AST/CST study, EQA proficiency programmes). • Cut-off thresholds for initiation of pre-emptive therapy are site-specific and vary significantly, therefore, difficult to compare clinical practice and develop standardised treatment models. • EBV Viral Load Standardisation Workshop (Third European Congress of Virology, Nürnberg, 2007) called for the development of an International Standard for EBV DNA.
Rationale 2 Variability in performance of EBV viral load assays Plasma spiked with Namalwa cells Clinical samples Log10 variation in reported results (relative to expected) Preiksaitis et al, Am J Transplant. 2009;9:269-79
Source material for EBV candidate Whole virus preparation of prototype laboratory EBV strain B95-8 Produced in cell culture, formulated in universal buffer and freeze dried Concentration of ~1x107 copies/mL (IU when established) ~5000 vials to be filled (August 2009)
Collaborative study protocol • Candidate standard to be evaluated alongside frozen liquid preparations: • B95-8 liquid bulk • EBV-positive Namalwa cells • EBV-positive Raji cells • ~30 participants (clinical and research labs, assay manufacturers) performing range of NAT-based assays • To ECBS 2010
Intended use Calibration of secondary references used in routine EBV viral load assays Calibration/validation of commercial NAT assays Evaluation of EBV-positive materials distributed in molecular quality assurance programmes