Download
1 / 30
350 likes | 647 Views
The Telephone. Dr Julian Tomkinson Nov 2012. Aims of session. Discuss use of telephone in general practice Look at some of evidence written Case scenarios / practice. Curriculum. 2.01 The GP Consultation in Practice

E N D
The Telephone Dr Julian Tomkinson Nov 2012
Aims of session • Discuss use of telephone in general practice • Look at some of evidence written • Case scenarios / practice
Curriculum 2.01 The GP Consultation in Practice Recognising how consultations conducted via remote media (telephone and email) differ from face-to-face consultations, and demonstrating skills that can compensate for these differences
Curriculum 3.03 Care of Acutely Ill People Communicate effectively with patients, relatives and carers over the telephone in order to accurately assess a patient who is acutely ill
Any worries about using the phone? Any help you need?
CSA The circuit of 13 cases in the CSA examination may include one telephone triage case New RCGP Building Euston Square
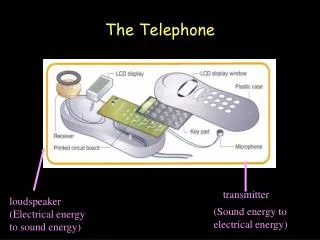
What do we use the telephone for? • To communicate with patients – in acute and follow-up situations • To communicate with other doctors and team members • Administrative tasks
Telephone use with patients • Straightforward consultation • To discuss results / prescription requests etc • For Triage • Review
Some statistics regarding telephone consultations • c.25% of primary care consultations are telephone based • Up to 55% of all OOH service calls are advice only. • In Bolton (where I do a weekly OOH shift) all OOH calls triaged by GP or Nurse
Benefits To the patient • Perceived as more convenient and quicker. • Easier access to self-care advice and • Increases access for who find getting to surgery difficult
Benefits To the doctor • Improving efficiency by moving the information instead of the patient • Triage - patients who need to be seen can be given appointments at times when demand is high • Can reduce workload - about 50% telephone consultations result in telephone advice alone.
GMC Guidance The GMC has emphasisedthat phone (or e-mail) should not diminish the quality of care patients receive. This is most likely to occur where: • The patient is not previously known to the doctor. • The assessment may be helped by examination. • There is little or no provision for appropriate monitoring of the patient or follow-up care.
What are the differences? Phone vs Face to face
Communication outcomes • More biomedical and less psychosocial or affective information is exchanged. • Shorter interactions account for variation seen in areas such as rapport building, patient education and counselling. • Doctors behave in a less patient-centred way on the telephone.
Circumstances surrounding use of phone Ideal situation Time to prepare and not doing anything else Opposite An interruption ie. doing something else / no preparation time
Suggested approach to a telephone consultation • Answer the telephone promptly. • State your name • Obtain caller's name and telephone number (in the event the patient has to be called back by another member of the team or the call becomes disconnected). • Speak directly with the person who has a problem. • Record date and time of call. • Record person's name, gender and age (obtain person's medical record, if available). • Take a detailed and structured history. (REMEMBER ICE) • Provide advice on treatment/disposition. • Specific advice regarding follow-up and when to contact a doctor. • Summarise and record the main points covered. • Request caller to repeat advice given (several times throughout the consultation). • Ask if the person has any outstanding questions or concerns. • Let caller disconnect first.
Training in telephone consultation skills should focus on • Active listening and detailed history taking • Frequent clarifying and paraphrasing (to ensure that the messages have been brought across in both ways) (chunking and checking) • Picking-up cues (eg pace, pauses, change in voice intonation) • Offering opportunities to ask questions • Offering patient education • Documentation
History • Chief complaint • What else is happening? • Character of symptoms • Onset • Duration • Location • Alleviating or worsening factors
DON’T FORGET TO DO WHAT YOU NORMALLY DO • PMH • Risk factors, e.g. Foreign travel • Pregnancy • Medications/otc • Allergies • Lives alone?
Things to remember • Ask if there is anything else worrying them • Be ready to take control ... nicely • Check that your final understanding of the problem matches yours. • Beware of previous assessments clouding your judgement but.... 2nd calls about same problem should be red flags. • Safety net with time frame, what to watch out for and ensure understanding. Who to call ?
Management Plan • Prepare to negotiate • Ambulance calling and refusal • Be ready with another plan if they disagree • Educate .. how long? What changes to look out for? • Meet anger with acknowledgement and calmness • RECORD EVERYTHING
Closure • Make sure not premature • Let the patient disconnect first • Everyone is clear on what happens next. • Eg in OOH setting • Advice? • Home visit? • Coming to centre? (+ where do they come)
Records • Document all incoming and outgoing calls with patients (and third party informants). Even brief contacts can be critical and note-keeping must be as reliable as for a face to face contact.
Appropriateness and safety • Always ask yourself, "Is telephone management appropriate in this situation?". • Revisit this question several times during the consultation. • As the assessment is based solely on the history, and the management plan cannot be reinforced with non-verbal cues, being systematic in covering all issues is especially important.
Medico-legal points • MPS report 22% of complaints about rudeness and attitude of clinician (lack of visual clues can make you sound rude) • Your duty of confidentiality means you need to ask yourself if you can guarantee any message you leave will remain confidential and will reach the patient • Take care speaking to / about patients on phone when away from work • Organise protected time and a confidential environment for telephone consultations
Check List • Prepare – gather info/breathe/ smile • Introduction • Check patient information • Find out what is happening – open start • Check patient’s thoughts, feelings and wishes(ICE) • Remember red flags • Formulate a diagnosis / strategy • Check / Safety net / Close • NOTES
References • Car J, Sheikh A; Telephone consultations. BMJ. 2003 May 3;326(7396):966-9. • GMC; General Medical Council; Providing advice and medical services on-line or by telephone; (1998); (pdf) • Males T, Telephone consultations in primary care: a practical guide. RCGP 2007. ISBN: 978-0-85084-306-4