Download
1 / 25
250 likes | 598 Views
Advanced Modes of CMV. RC 270. Pressure Support = mode that supports spontaneous breathing. A preset pressure is applied to the airway with each spontaneous inspiration. Pressure Support. Pure assist mode Patient determines rate, Vt, and inspiratory time Inspiration is flow cycled

E N D
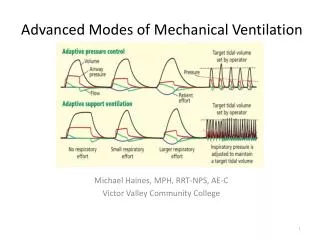
Advanced Modes of CMV RC 270
Pressure Support = mode that supports spontaneous breathing A preset pressure is applied to the airway with each spontaneous inspiration
Pressure Support • Pure assist mode • Patient determines rate, Vt, and inspiratory time • Inspiration is flow cycled • Most ventilators flow cycle a pressure support breath when inspiratory flow drops to 25% of the peak flow for that inspiration • PB 7200 flow cycles when pressure support flow drops to 5-10 lpm
Indications/Advantages: Pressure Support • Initially used to overcome the increased W.O.B. when breathing spontaneously through an E-T tube • Also may be used during spontaneous breaths during IMV • Weaning • Assisted ventilation (instead of A/C) • PSVmax
Initial Settings and Adjustments: Pressure Support • To overcome resistance of E-T tube, start at 5-10 cmH2O • For PSVMax, set pressure to level that gives an exhaled Vt of 10-12 ml/kg
Advantages: Pressure Support • Supports spontaneous breathing with decreased W.O.B.(with or without an E-T tube) • Can be done with a face mask • Usually less barotrauma and hemodynamic compromise • Patients like it!
Disadvantage: Pressure Support • A leak in the system prevents flow cycling • Will cause a CPAP effect
Pressure Controlled Ventilation (PCV) A set pressure is applied to the airway during inspiration and the breath time cycles
Pressure Controlled Ventilation • Can be used in A/C or control • Flow tapers – if it drops to zero before time cycling occurs, the pressure plateaus • Besides pressure, RCP also sets rate and either inspiratory time or I:E ratio • Vt may vary from breath to breath
Pressure Controlled Ventilation • Indications are same as for any type of CMV: • Apnea • Acute ventilatory failure • Impending ventilatory failure • Acute respiratory failure (Oxygenation failure) • Often used when volume cycling (volume control) is causing high airway pressures • Has been used to ventilate neonates since the 60s
PCV: Initial Settings and Adjustments • Initially choose a pressure (PIP) that gives desired exhaled Vt • If switching from volume cycling (volume control), use a PIP that is less than PIP during volume cycling • Adjustment in rate, PIP, and I:E (or inspiratory time based on ABGs, oximetry, and capnography • A change in PIP or I:E/insp time will change Vt
PC-IRV: Pressure Control with Inverse I:E Ratio Control mode only Patient is paralyzed Settings like PCV except for inverse I:E (gives long insp time)
PC-IRV used in diseases with high elastic resistance, eg ARDS Prolonged insp time helps O2 To increase PaO2: increase rate, PIP or insp time To decrease PaCO2: decrease rate or PIP
Airway Pressure Release Ventilation (APRV) Alternating levels of CPAP in a spontaneously breathing patient
APRV • Like PC-IRV but patient is breathing spontaneously and is not paralyzed • Also used for high elastic resistance • High CPAP level is applied longer than low CPAP level • Is NOT synchronized with inspiration and expiration
APRV: Settings and Adjustments • Low CPAP usually between 2-10 cmH2O • High CPAP usually between 10-30 cmH2O • RCP also sets the time for each CPAP level • Low CPAP is usually only for 1-2 seconds
Bilevel Positive Airway Pressure (BIPAP) IPAP + EPAP Differs from APRV – IPAP only during inspiration, EPAP only during expiration Rate and I:E ratio can also be set
Indications : BIPAP • Sleep apnea • Ventilatory Assist without intubation • Can be done via face mask • Often used to keep COPDers from being tubed and put on A/C • Popular mode for NIPPV (Non-invasive Positive Pressure Ventilation)
High Frequency Ventilation (HFV) A form of ventilation utilizing high rates and small Vt that seems to enhance diffusion of gases into and out of the lung
History of CMV HFV should not work based on classical respiratory physiology!
HFV: High Frequency Jet Ventilation (HFJV) • Vt usually 20-150 ml • Frequency (rate) 60-400 breaths per minute • Usually a catheter is inserted via ET tube or transnasally to apply jet bursts to airway • Adjust rate, driving pressure, and insp time, and FIO2
HFV: High Frequency Oscillation (HFO) • Vt between 5-50ml • Frequency between 400-3000 • Frequency expressed in Hertz (Hz) • 10 Hz equals 600 breaths per minute
Strict FIO2 and humidification can be variable Both appear to cause diffusion to occur from proximal airway to alveoli How does spontaneous breathing work? Coaxial flow Inspiration and expiration may be occurring simultaneously HFV seems to stimulate mucociliary clearance HFV (both HFJV and HFO)