Download
1 / 40
420 likes | 532 Views
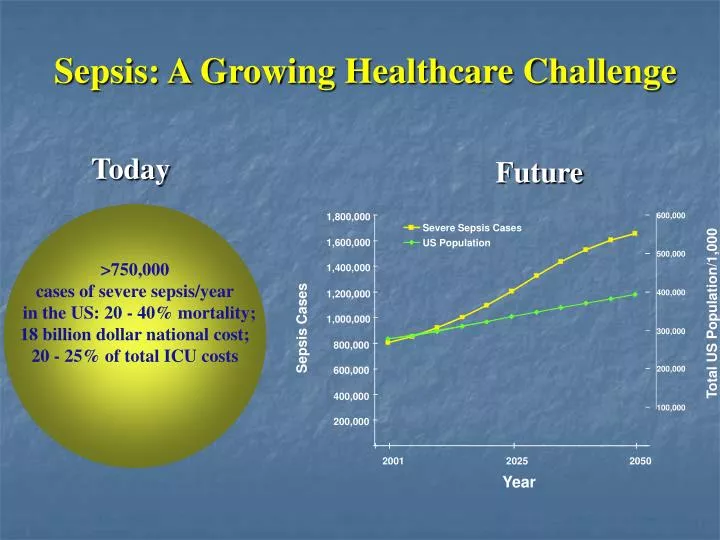
Future. 1,800,000. 600,000. Severe Sepsis Cases. 1,600,000. US Population. 500,000. >750,000 cases of severe sepsis/year in the US: 20 - 40% mortality; 18 billion dollar national cost; 20 - 25% of total ICU costs. 1,400,000. 1,200,000.

E N D
Future 1,800,000 600,000 Severe Sepsis Cases 1,600,000 US Population 500,000 >750,000 cases of severe sepsis/year in the US: 20 - 40% mortality; 18 billion dollar national cost; 20 - 25% of total ICU costs 1,400,000 1,200,000 400,000 Total US Population/1,000 1,000,000 Sepsis Cases 300,000 800,000 200,000 600,000 400,000 100,000 200,000 2001 2025 2050 Year Sepsis: A Growing Healthcare Challenge Today
Definitions: Sirs Host response to critical illness of either infectiousornoninfectious etiology. Defined by two or more: • T < 36 ° or > 38° • RR > 20 / min or PaCO2 < 32 • PR > 90 / min • WBC > 12,000/mm3 or < 4,000/mm3
Definitions SIRS: Host response to critical illness of either infectious or noninfectious etiology (defined by T°, HR, RR, WBC) Sepsis: SIRS due to a presumed or known site of infection Severe Sepsis: Sepsis with associated organ dysfunction Cardiovascular: SBP < 90 or 40 mmHg decrease Respiratory: Pa02/FiO2 < 250 in absence of pneumonia Respiratory: Pa02/FiO2 < 200 in presence of pneumonia Renal: UO < 0.5 cc/kg/hr Hematologic: Platelets < 100,000 or INR > 1.5 Acid-base: pH < 7.3 and lactate > 1.5 normal Hepatic, Central Nervous System Septic Shock:Sepsis with hypotension and perfusion abnormality (e.g. lactic acidosis, oliguria, acute alteration in mental status) unresponsive to adequate fluid resuscitation
High Risk Apache score > 25 Multiple Organ Failure Mechanical Ventilation Vasopressor Thrombocytopenia Shock DIC Low Risk Apache score < 25 Single Organ Failure No Mechanical Ventilation No Vasopressor No Thrombocytopenia No Shock “High Risk” versus “Low Risk” Populations
Goals of Management“Golden Hour” of care • “Maintain blood pressure through optimization of cardiac output and filling pressures” • Maintain adequate tissue oxygenation • Preserve vital organ function
SCCM Resuscitation Bundle • Element 1: Measure serum lactate • Element 2: Obtain blood cultures prior to antibiotics • Element 3: Antibiotics within 3 hours of ED admission, 1 hour of non-ED admission • Element 4: In the event of hypotension or increased lactate: Administer 20 ml/kg crystalloid • Vasopressors if not responsive to volume resuscitation • Element 5: Goal CVP of 8 / SVO2 of 70% or MVO2 of 65%
SCCM Management Bundle • Element 1: Low dose steroids in accordance with ICU policy • Element 2: Xigris in accordance with ICU policy • Element 3: Glycemic control (70 – 150) • Element 4: Low volume ventilation strategy (plateau pressure < 30 mmHg
Why Lactate? PDH
Lactate: Prognostic Value • Source doesn’t matter • High lactate a marker of severe physiological stress and risk of death • High lactate often not hypoxemia or hypotension related but reflects events at a cellular level.
Lactate Clearance and Survival • 111 patients admitted with sepsis • Average age 64.9 ± 16.6 • Apache Score 20.2 ± 6.8 • Severe sepsis 48% • Septic shock 52% • EGDT • Lactate Clearance: Lactate ED presentation – Lactate hour 6X 100 • Lactate ED presentation Nguyen HB. Critical Care Medicine: 2004:32;1637-1642
Lactate Clearance and Survival Nguyen HB. Critical Care Medicine 2004:32;1637-1642
Early Appropriate Antibiotic Administration: 2154 patients, 14 intensive care units Kumar A, et al. Critical Care Medicine 2006; 34: 1589 - 1596
The Goal of EGDT: Sv02 > 70% • Volume Resuscitation: 500-ml bolus of crystalloid every 30 minutes to maintain CVP 8 – 12 mm Hg. • Vasopressors/vasodilators to maintain MAP 65 – 90mm Hg • Transfuse to HCT of 30 percent • Dobutamine (2.5 – 20 μg/kg/min) until Sv02 = 70% • Intubation / ventilation / sedation if Sv02 not responsive to prior measures and remains< 70% Rivers, et al. NEJM 2001; 345:1368-1377
EGDT: Therapy Over First 72 Hours►Traditional ► EGDT * * * *
Definitions • Oxygen Delivery (~ 1,000 ml/min): • D02 = Ca02 x C.O. X 10 • Ca02 = (1.36 X Hb x Sa02) + .003 (Pa02) • D02 = [(1.36 X Hb x Sa02) + .003 (Pa02)] x C.O. X 10 • Oxygen Consumption (~ 250 ml/min): • V02 = C(a - v)02 x C.O. x 10 • Oxygen Delivery – Oxygen Consumption = Oxygen Extraction • Oxygen Extraction Ratio (OER): • V02 / D02
Oxyhemoglobin Dissociation • 97% of O2 bound to hemoglobin • Each RBC: 280,000,000 molecules of hemoglobin • Each molecule of Hgb: 4 O2 binding sites • CO: 240X affinity for Hgb than O2; shifts curve to left
Relative Effects of P02, Hgb, and C.O. on Oxygen Delivery D02 = [(1.36 X Hb x Sa02) + .003 (Pa02)] x C.O. X 10
Low Volume Ventilation: ARDSNet • Consortium of Clinical Centers Sponsored by NIH • Randomized controlled multi-center trial • 861 patients randomized to 6 ml/kg TV (Pplat<30cm) or 12 ml/kg TV • Trial stopped after 4th interim analysis due to significantly reduced mortality (30% vs 40%, p=0.005) • Increased organ failure-free days and lower IL-6 levels ARDS network N Engl J Med 2000;342:1301
Mortality / Ventilator Free Days ARDS network N Engl J Med 2000;342:1301
Corticosteroids in Sepsis • 1976: Schumer suggested that steroids improved survival in septic shock • Schumer, et al. Ann Surg. 1976;184: 333–341. • 3 mg/kg dexamethasone or 30 mg/kg methylprednisone • 1984: Sprung et al published a RCT using high dose steroids for septic shock • Sprung, et al. NEJM 1984:311;1137-1143. • early reversal of shock • similar hospital mortality • 1987: VA Cooperative Study • VA Study Group. NEJM 1987;317:659-665. • RCDBS, 112 steroid, 111 control • 30 mg/kg solumedrol + 5mg/kg/hr X 9 hrs • no difference in hospital mortality
CORTICUS Study • 499 patients • 1:1 randomization in block of 4 • 233 no ACTH response (< or = 9 mcg/dl post ACTH) • 125 hydrocortisone, 108 placebo • 254 ACTH response • 118 hydrocortisone, 136 placebo Sprung C et al. N Engl J Med 2008;358:111-124
CORTICUS Study Sprung C et al. N Engl J Med 2008;358:111-124
CORTICUS Study • “On the basis of these findings, hydrocortisone cannot be recommended as general adjuvant therapy for septic shock (vasopressor responsive), nor can corticotropin testing be recommended to determine which patients should receive hydrocortisone therapy. Hydrocortisone may have a role among patients who are treated early after the onset of septic shock who remain hypotensive despite the administration of high-dose vasopressors (vasopressor unresponsive).” Sprung C et al. N Engl J Med 2008;358:111-124
Protein C: Sepsis is a thrombotic as well as inflammatory disorder • Vitamin K-dependent protein synthesized in the liver • Normally activated on endothelial surface when thrombin binds to thrombomodulin (EPCR) • Inactivates factors Va and VIIIa, limiting the generation of thrombin • Inactivates PAI-1, thereby having profibrinolytic activity • Inhibits the production of inflammatory cytokines (TNF- , interleukin-1, and interleukin-6) by macrophages
Intensive Insulin Therapy in the Critically ill • Hyperglycemia and insulin resistance are common • In diabetic patients with AMI keeping blood glucose < 215 mg/dL improves long term outcomes • van den Berghe et al conducted a RCT of 1548 patients to evaluate role of intensive versus conventional glycemic control in critically ill Van den Berghe et al NEJM 2001: 345; 1359-67
Trial design • 1548 patients admitted to surgical ICU, mechanically ventilated • All patients received 200-300g glucose/day on admission • TPN or parenteral fluid within 24 hours of admission with 60 - 80% glucose calories • Conventional: titrate glucose to 180-200 mg/dL • Intensive: titrate glucose to 80-110 mg/dL Van den Berghe et al NEJM 2001: 345; 1359-67
Role of Intensive Insulin • At 12 months intensive insulin reduced mortality by 3.4% (p<0.04) • Intensive insulin resulted in: • 34% decrease in in-hospital mortality (10.9 7.2) • No difference in mortality for ICU stay < 5 days • 42% reduction in ICU deaths (8.0 4.6) • Reduction in ICU sepsis-related deaths (33 8) • 46% reduction in bloodstream infection (7.8 4.2) • 41% reduction in renal failure requiring RRT (8.2 4.8) • 50% decrease in median RBC transfusions (2 1) Van den Berghe et al NEJM 2001: 345; 1359-67
Trial design • 1200 patients admitted to medical ICU • 22 – 30 kilocalorie/kg weight, enteral feeding ASAP • Conventional: titrate glucose to 180-200 mg/dL • Intensive: titrate glucose to 80-110 mg/dL Van Den Berghe, et al. NEJM 2006: 354; 449-461.
Role of Intensive Insulin “ .. the benefit from intensive insulin therapy requires time to be realized. Indeed, the intervention is aimed not at curing disease but at preventing complications that occur during and, perhaps in part as a result of, intensive care. “ Van Den Berghe, et al. NEJM 2006: 354; 449-461.
IIT: Unknowns • Optimal Blood Sugar • ? 80 – 110 • ? 140 – 180 • ? < 200 • ? Timing of initiation of IIT • Risk of hypoglycemia • Risk / benefit ratio
Conclusion • Sepsis bundle can be useful in standardizing care and minimizing variance • Lactate can provide diagnostic and prognostic information • Early antibiotic administration essential • Early volume resuscitation essential • No ideal pressor • Low volume ventilation strategy useful • Data on steroids / Xigris less compelling • Glycemic control useful (more so in surgical than medical populations)
Effects of rhAPC on 28-day mortality in patients with severe sepsis
Meta-analysis of effects of rhAPC on 28-day mortality in patients with severe sepsis and APACHE II score of < 25
Meta-analysis of effects of rhAPC on 28-day mortality in patients with severe sepsis and APACHE II score of > 25