Download
1 / 30
410 likes | 1.76k Views
Radiology of Connective Tissue Disease associated Interstitial Lung Disease . John Murchison. Why do HRCT?. Superior to CXR and conventional CT at showing parenchymal abnormalities With MDCT all CT chests are effectively HRCT. Indications for HRCT. Is lung disease present?

E N D
Radiology of Connective Tissue Disease associated Interstitial Lung Disease John Murchison
Why do HRCT? • Superior to CXR and conventional CT at showing parenchymal abnormalities • With MDCT all CT chests are effectively HRCT
Indications for HRCT • Is lung disease present? • What is the nature of the abnormality? • Are changes acute or chronic? • Follow up to assist management • Selection of biopsy site
Indications for HRCT • Is lung disease present? • Much more sensitive at assessing lung parenchma than CXR • Superimposed structures • ? Normal ? Abnormal • PFT abnormalities and apparently normal CXR • Is further management required? • Or no need eg emphysema
Indications for HRCT • What is the nature of the abnormality? • Sometimes able to give a specific diagnosis • Bronchiectasis, UIP, emphysema • Narrows the differential diagnosis • Appropriate selection of further tests
Indications for HRCT • Are changes acute or chronic? • Chronic eg fibrosis • Acute ground glass • Follow up to assist management • Has disease progressed / improved? • Selection of biopsy site • Many diffuse lung diseases have a patchy distribution. Select active disease • Avoid end stage fibrosis
Scanning Variants • Supine scan- standard • Prone scan • Expiratory scan
Scanning Variants supine • Prone scan- • dependant changes often seen particularly at lung bases • If concern that may be obscuring early fibrosis or that changes may not be genuine do prone scan prone
Scanning Variants supine • Prone scan- • dependant changes often seen particularly at lung bases • If concern that may be obscuring early fibrosis or that changes may not be genuine do prone scan prone
Scanning Variants Inspiration • Expiratory scan • Demonstrates air trapping • If concern re obstructive lung disease eg PFTs • Hyperlucency on HRCT • If particularly looking for conditions where air trapping likely eg Bronchiolitis obliterans • In normal patients HU increases uniformly on expiration • If air trapping HU remains low Expiration
Patterns of air space opacification consolidation ground glass
Ground Glass ground glass attenuation Ground glass attenuation may be correlate with a) evidence of interstitial inflammation with airspace filling by macrophages b)patchy fibrosis or c) a combination of above.
HRCT features of fibrosis, Intra-lobular and inter-lobular septal thickening, walled cysts representing honeycombing, may be associated traction bronchiectasis
DPLD Diseases of known cause or association Granulomatous diseases Idiopathic interstitial pneumonias Others Eosinophilic diseases UIP Sarcoidosis Connective tissue diseases NSIP Rare diseases Drug-induced diseases AIP Pneumoconiosis RB-ILD DIP LIP Asbestosis COP IPF / CFA Hypersensitivity pneumonitis
CXR-UIP Initially ill-defined or ground-glass opacities, peripheral reticular opacities, As disease progresses reticular pattern becomes coarser, most marked at bases, often volume loss, end stage diffuse honeycombing.
HRCT 1) features of fibrosis, Intralobular septal thickening, walled cysts representing honeycombing, may be associated traction bronchiectasis 2)ground glass attenuation common but usually less than reticular abnormalities. Ground glass attenuation may be correlate with a) evidence of interstitial inflammation with airspace filling by macrophages b)patchy fibrosis or c) a combination of above. 3)characteristically aperipheral basal distribution
Sarcoid Drugs IPF Asbestosis NSIP DIP RBILD COP EAA UIP CTD • Radiological differential diagnosis in ‘IPF’ • An HRCT that predominantly shows bibasal honeycombing is virtually 100% specific for UIP. • The HRCT pattern of UIP found in IPF can be indistinguishable from that seen in asbestosis, collagen vascular disease or as a response to drugs. • Patients with chronic hypersensitivity pneumonitis or with end-stage sarcoidosis can uncommonly develop a CT pattern similar to UIP
CXR NSIP bilateral pulmonary infiltrates. Lower lung zones more frequently involved.
HRCT NSIP • 1) ground glass predominant finding in most cases and sole finding ~50%. • 2) Irregular linear or reticular opacities seen about 50% cases. May be traction bronchiectasis. • 3) Honeycombing and consolidation relatively infrequent • 4) Bilateral symmetrical basal predominance
NSIP radiological differential diagnosis • Depends on the predominant pattern exhibited. • Experienced radiologist found it indistinguishable from • UIP 32% • Hypersensitivity pneumonitis 20% • Organising pneumonia 14% • Other diagnosis 12% Radiology 2000 vol 217
Extent and Distribution of disease UIP /NSIP • Feature NSIP UIP p value • Disease extent (%) 37.1 +/- 22.7 44.0 +/- 23 .29 • Ground glass (%) 47.4 +/- 27.2 26.7+/- 22.5 <.005 • Coarseness score (max 15) 6.0 +/- 3.1 8.3+/- 2.9 .01 • Subpleural distribution (%) 60 71 .08 • Basal distribution (%) 62 70 .25 • Bronchocentric distribution 5 9 .29 53 patients Macdonald et al Radiology 2001: 221
COP radiology • Patchy non-segmental, unilateral or bilateral areas of air space consolidation. • Often vary in site and configuration over time. • May be irregular reticular opacities. Rarely a major feature. • Small nodular opacities usually with other features but occasionally on their own
COP • HRCT findings • 1 Bilateral Air-space Consolidation 80% • 2 Ground glass opacities 60% • 3 Subpleural and/or peribronchovascular distribution • 4 Bronchial wall thickening, dilatation in abnormal areas • 5 Small nodular opacities often peribronchiolar (30-50% of cases) • 6 May get irregular reticular opacities • 7 Combination of findings in 1 and 2
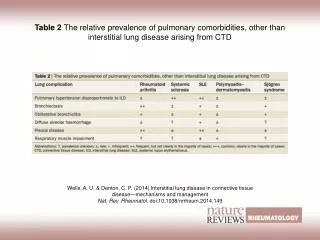
HRCT Rheumatoid Arthritis • HRCT patterns • UIP/ NSIP • COP • Brochiolitis obliterans • Necrobiotic nodules • Pleural thickening/ effusions
Scleroderma.(PSS) • High prevalence of pulmonary involvement • HRCT patterns • Pulmonary arterial hypertension( 50%) • ILD ( 80%) usually NSIP • Pleural thickening /effusion • Oesophageal dilatation.
CXR and CT clues • Joint abnormalities particularly AC and shoulder joints with Rheumatoid arthritis • Dilated oesophagus suggest scleroderma or variant • Pulmonary artery enlargement out of proportion to lung parenchymal changes may reflect vaculopathy especially scleoderma • Soft tissue calcification –dermatomosytis or scleroderma • Multiple compartments think RA
Radiology of Idiopathic ILD • The lung has a limited number of patterns of response to injury and there is often a lack of correlation between aetiological insult and radiological appearance of the lung • We need to recognise that in many cases there is not a clear cut match between the ‘clinical syndrome’ and the ‘radiological pattern’ of disease • The latter may be more important in determining prognosis • Patients are managed in a multi-disciplinary manner in order to reach a final clinical diagnosis
Drug treatment • Gold usually diffuse alveolar infiltrates- can look like OP • Methotrexate- • can produce sub-acute hypersensitivity- centilobular ground glass • Pneumonitis –more likely if pre-existing ild • D-penacillamine- constrictive bronchiolitis • Non -steroidals – hypersensitivity • Salicylates OD pulmonary oedema • Opportunist infections • Increased risk lymphoma and lung cancer