Download
1 / 36
360 likes | 424 Views
Infectious myositis is an uncommon infection of skeletal muscle, often caused by bacteria or viruses. Learn about bacterial pyomyositis, Streptococcus myonecrosis, and Clostridium myonecrosis, along with their clinical presentations and management strategies. Explore the pathophysiology of tetanus and the forms of this condition.

E N D
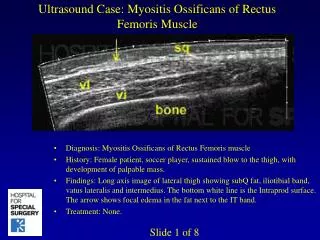
Infectious Myositis: Infectious myositis is an uncommon acute, or chronic infection of skeletal muscle. Most often seen in youngadults. The mostcommon infectious agent is the bacterium, Staphylococcus aureus (77-90%of Myositis cases)(prevalent in tropicalcountries). Viruses, other bacteria (including Mycobacteria), fungi, and parasites can cause myositis. It consists of a primary abscess, edema, and hypoechoicinflammatory Mass.
a Viraletiologies typically cause diffusemyositis, whereas bacteria and fungi usually lead to a localmyositis which may be associated with sites compromised by trauma or surgery and are more common among immuno-compromised patients. Localized collections within the muscles are referred to as pyomyositis. Other pyogenic causes of myositis include gasgangrene, groupAStreptococcalmyonecrosis, and other types of non- Clostridial myonecrosis.
Bacterial pyomyositis: Pyomyositis consists of a primarymuscleabscess and is prevalent in tropical countries. It is associated mainly with immunocompromisedpatients, and intravenousdrugabusers who traumatically contaminate their muscles with foreign material. The clinicalpresentation is often nonspecific with muscleachesand a deep induration. This may at first suggest an intramuscular neoplasm. The causative agent is Staphylococcus aureusin over 90% of cases.
StreptococcusMyonecrosis: -Streptococcalmyositis is a rare, often fatal, acute infection of the muscle, caused by an invasivegroupAbeta-haemolytic Streptococcus. -It is characterized by muscle necrosis without abscess formation, and, in contrast to necrotizingfasciitis, does not primarily affect the subcutaneous tissue or skin. -It is a predisposing factor or septicshock. -Management: high-dose intravenous antibiotics. intensive fluid and nutritional support. Streptococcal toxic shock syndrome.
ClostridiumMyonecrosis: (Gas gangrene): ClostridialMyonecrosis is a bacterial infection that produces gas (tissues) in gangrene (necrotic damage of tissue specifically muscles). It is a deadly form of gangrene usually caused by Clostridiumperfringensbacteria. This bacterium causes Myonecrosis via specificexotoxins . -In general, different clostridium species are opportunistic and enter the body via significant skin breakage. The exotoxin is commonly found in C. perfringenstype A strain and is known as alpha toxin.
a The alphatoxin is a phospholipase requiring zinc for activation. First, The C-terminaldomainbindscalcium and allows the toxin to bind to the phospholipid head-groups on the cellsurface. The N-terminaldomain has phospholipase activity. This property allows hydrolysis of phospholipids such as phosphatidylcholineto diacylglycerol.
N The end result includes activation of arachidonic acid pathway and production of thromboxaneA2 (vasoconstrictor), production of IL-8, platelet-activatingfactor, and several intercellular adhesionmolecules. These actions combine to cause edema due to increased vascular permeability.
Clinical presentation of Clostridium perfringens infection: a
Tetanus ( lockjaw disease): It is a medical condition characterized by a prolongedcontraction of skeletalmusclefibers. The primary symptoms are caused by tetanospasmin (A-light chain, B-heavy chain), a neurotoxin produced by the Clostridiumtetani. Infection occurs through wound contamination and often involves a cut or deep puncture wound.
N - As the infection progresses, musclespasms develop in the jaw and elsewhere in the body. - Mortalityrates reported vary from 48% to 73%. - In recent years, approximately 11% of reported tetanus cases have been fatal. Pathophysiology: - Tetanus begins when endospores of Clostridiumtetani enter damaged tissue. - The spores transform into rod-shaped bacteria and produce the neurotoxintetanospasmin. - This toxin is inactive inside the bacteria.
N When the toxin is released , it will be activated by proteases. Active tetanospasmin enters at neuromuscularjunctionsof motor neurons, B-chain (heavy) binds to neuronal membrane sphingolipid. The light-Achaincarried by axonal transport of peripheral nerve terminals to cellbodies in the spinalcord and brainstem where it binds to receptors at these sites.
a -The A-chain, a zincendopeptidase, attacks the vesicle-associated membrane protein ( synaptobrevin) of centralnervoussystemneurons. -The action of the A-chain stops the affectedneurons (inhibitory synapses)from releasing the inhibitoryneurotransmittersGABA (gamma-aminobutyric acid) and glycine. -Consequence dangerousoveractivityin the muscles from the smallest stimulus. Clostridiumtetanialso produces an oxygen-labile hemolysincalled tetanolysinthat destroy the muscle protein.
Forms of tetanus: Generalized tetanus: It is the most common type of tetanus, representing about 80% of cases. The generalized form usually presents with a descending pattern. The first sign is lockjaw, and the facialspasms called risussardonicus( Sardonic smile), followed by stiffness of the neck, difficulty in swallowing, and rigidity of pectoral and calf muscles.
N Other symptoms include elevatedtemperature, sweating, elevatedbloodpressure, and cardiacarrhythmias. Other forms: Neonatal , localized and cephalic tetanus.
Clinical presentation of Clostridium tetani: Muscle spasms in a patient suffering from tetanus. Neonatal Tetanus. Painting by Sir Charles Bell, 1809. Facial spasms called RisusSardonicus- First Symptom of Generalized Tetanus.
Laboratorydiagnosis: Clinical specimens: Pus swab, exudate (thioglycolate media). C. perfringens:Beta surrounded Beta hemolytic filamentous by Alpha hemolysis. C. tetani.
Parasitic Myositis: Trypanosomacruzi: Transmission : when the Winged bug of the genus Triatoma deposits feces on the skin surface and subsequently bites; the human host. Late ( chronic) stage infection: affects the nervous system, digestive system and cardiac muscle. The protozoa will infect Skeletalmuscle by its Amastigote stage. Amastigote stage in skeletal muscle.
Trichinellaspiralis: It is a nematode parasite, occurring in rats, pigs, and humans, and is responsible for the disease trichinosis. Humans typically become infected when they eat improperly cooked pork (Trichinellainfected) meat. Female Trichinella worms stay for about six weeks, in small intestine, and in that time can produce up to 1,500 larvae. Larvae will migrate with blood to striatedmuscles causing myositis. The muscles invaded mainly are: pectoral muscles, tongue, and the gastrocnemius.
Cysticercosis: Cysticercosis involves infection of individuals with the larval stage of Taeniasolium, the cysticerci, which normally infects pigs. Autoinfection may occur due to fecal-oral transmission. The oncosphere( hexacantho-embryo) penetrates the intestinal wall and migrates in the circulation to the tissue ( skeletalmuscles).
Rabies: Virology: The rabies virus is the type species of the Lyssavirusgenus, in the family Rhabdoviridae. Lyssaviruses have helicalsymmetry, with a length of about 180nm and a cross-sectional diameter of about 75nm. These viruses are enveloped and have a single-strandedRNAgenome Electron microscopy Show the helical Enveloped single stranded RNA virus.
a Rabies is a viral disease that causes acute encephalitis (inflammation of the brain) in warm-bloodedanimals. The virus is usually present in the nerves and saliva of a symptomaticrabidanimal. The route of infection usually, but not always, is the animal bite.
N The infection is initiated by inoculation of virus into skeletalmuscles, virus will be replicated in muscle and transferred to peripheralnervoussystem. The rabies virus travels to the brain by following the peripheral nerves. Rabies kills around 55,000 people a year, mostly in Asia and Africa (2010).
a a
Osteomyelitis: Osteomyelitis is the infection of the bone or bone marrow. It can be classified on the basis of the causative organism (pyogenic bacteria or mycobacteria), the route, duration and anatomic location of the infection. Pathogenesis: Microorganisms may infect bone through one or more of three basic methods: via the bloodstream, from localareas of infection (as in cellulitis), penetrating trauma, jointreplacementsor internal fixation of fracturesor root-canaled teeth.
A Once the bone is infected, leukocytes enter the infected area, and engulf the infectiousorganisms, release enzymesthat are associated with bone lyses. Pus spreads into the bone's blood vessels, impairing their flow, and cause necrotic dead area of the bone called sequestra,form the basis of a chronic infection. Often, the body will try to createnewbone around the area of necrosis. The resulting newbone is often called an involucrum.
Septic arthritis: Septic arthritis is the invasion of a joint by an infectious agent which produces arthritis. People with artificial joints are more at risk than others. Septic arthritis is considered a medical emergency. If untreated, it may destroy the joint in a period of days. The infection may also spread to other parts of the body.
Prevalence, and pathogenesis: The incidence of septic arthritis has been estimated at 2 to 10 cases per 100,000 in the general population, and as high as 30 to 70 cases per 100,000 in patients with rheumatoid arthritis. Pathogenesis: -Routes of Entry: 1- Dissemination of pathogens via the blood. hematogenous 2- From contaminated needle. 3- Dissemination from soft tissue infection, entry via penetrating trauma.
a -Primary infection: -The Synovial A cell (APC) engulfs the microbe. - Production of TNF, IL-8, and PLAF. - Chemotaxis, cellular infiltration, and edematous edema. - Toxic free radicals production. - Proteoglycan and collagen destruction, cartilage destruction. - Direct pressure necrosis, more cartilage destruction. - Specific T-cell response, and Polyclonal B cell activation. Secondary: Osteomyelitis.
a Bacteria that are commonly found to cause septic arthritis are: 1-Staphylococcusaureus- the most common cause in adults; (40-50% of cases). Others: 10-20%: 2-Streptococci- the second most common cause 3-Haemophilusinfluenzae- was the most common cause in children but is now uncommon in areas where Haemophilus vaccination is applied. 4-Neisseriagonorrhoea- in young adults 5-Escherichiacoli- in the elderly, IV drug users and the seriously ill.
Signs and Symptoms of Septic arthritis: Patients with septic arthritis usually present with : 1-Joint pain. 2-Redness over the joint. 3-Joint inflammation and swelling. 4-Synovial fluid accumulation. Synovial fluid analysis: 1- Physical examination: The normal appearance of a sample of synovial fluid is usually: A-Straw colored. B-Clear. C-Moderately Viscous.
A Changes in the physical characteristics may provide clues to the disease present such as: A-Less viscous fluid may be seen with inflammation. B-Cloudy synovial fluid may indicate the presence of microbes, white blood cells, or crystals. C-Reddish synovial fluid may indicate the presence of blood.
N 2-Chemical examination: A-Glucose: typically lower than blood glucose levels. -Could be significantly decreased with joint inflammation and infection. B-Protein: increased with bacterial infection. C- Lactate dehydrogenase: -increased LD (LDH) level may be seen in rheumatoid arthritis, infectious arthritis. D-Uric acid—increased with gout.
N 3-Microscopic examination : Normal synovial fluid has small numbers of white blood cells (WBCs) and red blood cells (RBCs) but no microorganisms or crystals present. Specimens should be concentrated by centrifugation for: A-Total WBCs count: could be elevated. B-Differential count: Neutrophils increased with bacterial infection. Eosinophils elevated in Lyme disease.
N C-Gram’s stain: for detection of Gram-positive and negative bacteria. D-AFB (Z.N stain) smear: for Mycobacteriumtuberculosis. 4-Culture and sensitivity test: specimens should be cultured on blood and chocolate agar and incubated at aerobic and anaerobic (10%CO2) conditions respectively. Neisseria and Haemophilus species grow only on chocolateagar.