Download
1 / 24
240 likes | 672 Views
All Children Should Be Anaesthetised in a Children’s Hospital. Dori Ann McCulloch MidStaffordshire Hospital NHS Foundation Trust Paediatric Anaesthetic Network June 2010. WHY?!?. Why not?!?. Report of the National Confidential Enquiry into Perioperative Deaths, 1989

E N D
All Children Should Be Anaesthetised in a Children’s Hospital Dori Ann McCulloch MidStaffordshire Hospital NHS Foundation Trust Paediatric Anaesthetic Network June 2010
Why not?!? • Report of the National Confidential Enquiry into Perioperative Deaths, 1989 • Deaths in hospitals of children under the age of 10 years • J Lunn 1992 Paediatric Anaesthesia • “Implications of the National Confidential Enquiry into Perioperative Deaths for paediatric anaesthesia”
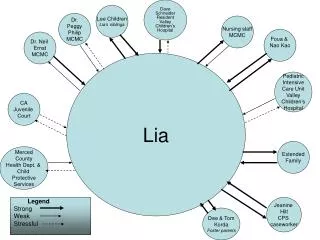
Frequency of current experience for a children’s anaesthetist
What’s been happening since then? • Various interpretations • Many articles • Thousands of words • Meetings and meetings • And then, standards
Editorial • Tomlinson A, Anaesthetists and care of the critically ill child, Anaesthesia Volume 58 Issue 4, p309-311. • Some hospitals refuse to anaesthetise under two’s • Some anaesthetists refuse to treat or anaesthetise children of varying ages • Some surgical departments refused to do emergencies in children
Good Surgical Practice • 2008 document • Royal College of Surgeons of England
Good Surgical Practice “Surgeons must treat children only if they have the appropriate training and ongoingexperience in the clinical care of children in their speciality, except in the case of emergency.” “Surgeons must demonstrate competence in their own area of practice and a willingness to refer where necessary.”
Good Surgical Practice • 13 general bullet points to meet standards • Working with children • Specialised communication with children • Be aware of the needs and welfare of children • Communicate effectively with parents • Protect the child’s privacy • Treat children only if appropriately trained and ongoing experience
The Tanner Report • ? New puberty guidelines? • “A team response to the acutely or critically sick or injured child in the district general hospital” • Department of Health, A team response • October 2006
Working Group, or TEAM • Royal College of Paediatrics and Child Health • Royal College of Anaesthetists • Association of Paediatric Anaesthetists • Children’s Surgical Forum of the Royal College of Surgeons • British Association of Paediatric Surgeons • Royal College of Nursing • Department of Health • a parent
The Tanner Report • Six generic skills • Recognise the critically sick or injured child • Initiate appropriate immediate treatment • Work as part of a team • Maintain and enhance skills • Be aware of issues around safeguarding children • Communicate effectively with children & carers
Tanner, continued • Skills maintenance including specialised courses, in house courses, personal practice, logbook proof of competency • Anaesthetists with limited ability to maintain his/her skills may benefit from an attachment to a larger centre.
Tanner, continued • Emergency surgery in children should only take place in hospitals that have inpatient children’s facilities and that provide elective surgical care
Improving services for children in hospital • Healthcare Commission Document • Report of the follow-up to the 2005/06 review • March 2009
Restrictions! • Child protection training for nurses, consultant surgeons & consultant anaesthetists in emergency care & day case care • Managing pain & administration of analgesia by nurses in emergency care and day case care (?!?)
More restrictions • Training in life support for nurses, consultant surgeons and consultant anaesthetists • 26% currently successful • Maintaining the skills of appropriately experienced staff in outpatient and surgical settings • 28% currently successful
Conclusions, or more numbers • Surgeons • Consultant surgeons carrying out insufficient levels of work on children, less than 100 finished consultant episodes in a year • Anaesthetists • By inference suggest each consultant anaesthetist should anaesthetise 21 children in a year aged 29 days to 12 years
In conclusion • “The results of anaesthesia and surgery for children in the United Kingdom are very good.” • Lunn JN. Implications of the National Confidential Enquiry into Perioperative Deaths for paediatric anaesthesia. Paediatric Anaesthesia 1992
Sources • Royal College of Surgeons of England, Surgery for Children: Delivering a First Class Service (Report of the Children’s Surgical Forum), July 2007 • Department of Health, The Acutely or Critically Sick or Injured Child in the District General Hospital: A Team Response, 2006 • Lunn JN, Implications of the National Confidential Enquiry into Perioperative Deaths for paediatric anaesthesia, Paediatric Anaesthesia 1992; 2:69-72. • Paediatric Surgery conference 2010 • Tomlinson A, Anaesthetists and care of the critically ill child, Anaesthesia Volume 58 Issue 4, p309-311.