Download
1 / 26
270 likes | 389 Views
Country Experience I nforming F easibility. Implementing Option B+: Malawi. Option B+ (Malawi) . Tenofovir phase in 1 st line( Zambia). Accelerated global phasing out of d4T. d4T phase out in HIV programmes. Raising CD4 threshold to 350 cells (Ethiopia).

E N D
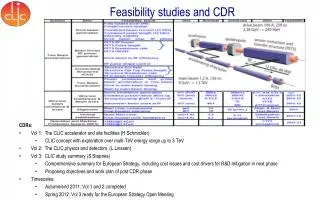
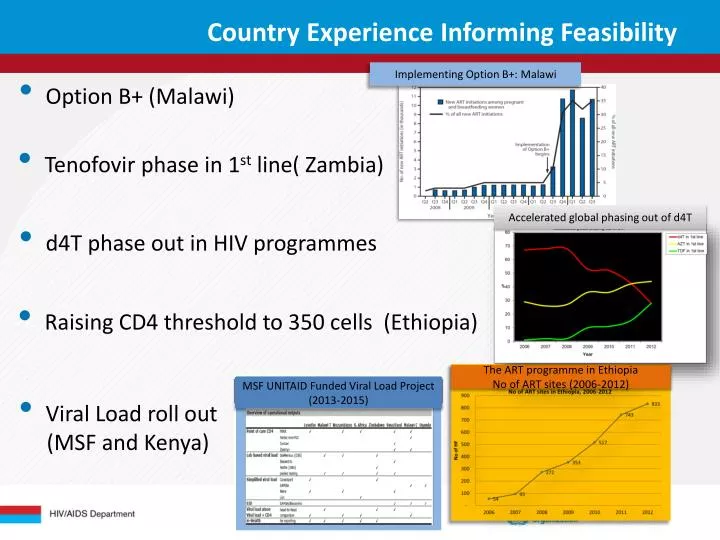
Country Experience Informing Feasibility Implementing Option B+: Malawi • Option B+ (Malawi) • Tenofovir phase in 1st line( Zambia) Accelerated global phasing out of d4T • d4T phase out in HIV programmes • Raising CD4 threshold to 350 cells (Ethiopia) The ART programme in Ethiopia No of ART sites (2006-2012) MSF UNITAID Funded Viral Load Project (2013-2015) • Viral Load roll out • (MSF and Kenya)
2013 ARV Guidelines: Highlights • OVER 50 NEW RECOMMENDATIONS • Clinical • Operational and Service Delivery • HIV testing & counselling TABLES, CHECKLISTS & ALGORITHMS ICONS FOR TARGET POPULATIONS ADDITIONAL SUMMARY BRIEFS (15 PAGES) ICONS FOR NEW RECOMMENDATIONS 6 CHAPTERS: ALONG THE CONTINUUM OF CARE
Key Themes of New Recommendations Clinically relevant • Earlier initiation of ART (CD4 ≤ 500) • Immediate ART for children below 5 years • ART initiation for all pregnant and breastfeeding women (Option B/B+) and lifelong ART (Option B+) • Harmonization of ART across populations (e.g., adults and pregnant women, Option B/B+) and age groups • Simplified, fewer, and less toxic 1st-line regimens (TDF/XTC/EFV) Operationally relevant • Use of Fixed Dose Combinations as a preferred approach • Improved patient monitoring to support better adherence and detect earlier treatment failure (increased use of VL) • Recommend task shifting, decentralization, and integration • Community based testing to complement broader HTC
What are the components of Guidance for Programme Managers? 1. Examine key parameters for decision making Discuss key data needed for evidence-based decisions Design an inclusive and transparent process Discuss implementation considerations Review tools for costing and planning
Summary of Changes in Recommendations: When to Start in Adults
Evidence Summary: When to Start in Adults • Systematic Review of 24 studies (3 RCTs, 21 observational ) • Multiple countriesthroughout Europe, North America, Central & South America, sub-Saharan Africa and Asia-Pacific • Outcomes reported: • mortality • progression to AIDS • progression to AIDS or death • non-AIDS defining cancer • serious non-AIDS events • CD4 increase • viral suppression, failure, rebound • SAE and grade 3 or 4 lab abnormalities
Evidence Summary:Risk of Death and/or Progression to AIDS RCTs – SMART / HPTN 052 Observational data Risk of Death or Progression to AIDS Clinical Trials (RCTs) Low quality evidence for lower risk of progression to AIDS or death with early ART (2 RCTs) Observational studies Moderate quality evidence for lower risk of death (13 studies) or progression to AIDS (9 studies) with early ART Risk of Death Risk of Progression to AIDS
Evidence Summary:Risk of HIV Sexual Transmission Clinical Trial - HPTN 052 Observational data RCT to examine efficacy of ART in preventing HIV transmission between discordant couples HIV+ partner had CD4 ≥ 350-550 cells/µL and was randomized to early vs. delayed ART Significant HIV prevention benefit – a 96% reduction in transmission. 1 genetically linked infection in early ART arm versus 29 infections in delayed arm. Early ART Late ART RCT and Observational data • High to moderate quality evidence that treatment prevents sexual transmission of HIV (1 RCT and observational data)
Populations With No Specific Recommendations • Insufficient evidence and/or favorable risk-benefit profile for ART initiation at CD4 > 500 cells/mm3 (or regardless of CD4 count) in the following situations: • Individuals with HIV who are 50 years of age and older • Individuals co-infected with HIV and HCV • Individuals with HIV-2 • Key populations with a high risk of HIV transmission (e.g.: MSM, sex workers, IDU) These populations should follow the same principles and recommendations as for other adults with HIV
Summary of Changes in Recommendations: What to Start in Adults
Rationale: One Regimen For All Preferred 1st line regimen: TDF + 3TC (or FTC) + EFV • Simplicity: regimen is very effective, well tolerated and available as a single, once-daily FDC and therefore easy to prescribe and easy to take for patients – facilitates adherence • Harmonizes regimens across range of populations (Adults, Pregnant Women (1st trimester), Children >3 years, TBand Hepatitis B,) • Simplifies drug procurement and supply chain by reducing number of preferred regimens (phasing out d4T) • Safety in pregnancy • Efficacy against HBV • EFV is preferred NNRTI for people with HIV and TB (pharmacological compatibility with TB drugs) and HIV and HBV coinfection (less risk of hepatic toxicity) • Affordability (cost declined significantly since 2010)
Evidence Summary: What to Start Immunologic Response (48 weeks) • Systematic review (10 RCTs): TDF+3TC (or FTC)+EFV superior vs. other EFV containing regimens and vs. TDF/3TC+ PI/r on major outcomes - occurrence of SAEs, virologic and immunologic response (high to moderate quality of evidence) • Systematic review (7 RCTs, 27 observational): NVP > 2 fold more likely to be discontinued due any adverse effect compared to EFV (moderate to low quality of evidence) • Systematic review of preclinical data (5 studies): support pharmacological equivalence interchangeability of 3TC and FTC (low quality evidence) Virologicalresponse (48 weeks) Severe adverse events (48 weeks) Discontinuation NVP vs. EFV Comparative efficacy 3TC and FTC
Evidence Summary: Safety of EFV and TDF in Pregnancy EFV TDF No increased risk of birth defects with EFV when compared with other ARVs • Potential concerns include renal toxicity, adverse birth outcomes and effects on bone density • Systematic review assessed the toxicity of fetal exposure to TDF in pregnancy • In Antiretroviral Pregnancy Registry, prevalence of all birth defects with TDF exposure in 1st trimester was 2.4% (same as background) • Limited studies showed no difference in fetal growth between exposed/unexposed • No studies of TDF among lactating women, who normally have bone loss during breastfeeding • Current data reassuring • More extensive studies ongoing • Systematic review (including Antiretroviral Pregnancy Registry), reported outcomes for 1502 live births to women receiving EFV in the first trimester and found no increase in overall birth defects • Excludes > 3 fold increased risk in overall birth defects Source: Ford N et al. AIDS, 2011. Ford N et al. AIDS, 2013. Ekouevi DK et al.J AIDS, 2011. WHO, Geneva Use of EFV during pregnancy. 2012. http://www.who.int/hiv/pub/treatment2/efavirenz/en Nightingale SL. JAMA, 1998. British HIV Association. Guidelines for the management of HIV infection in pregnant women. HIV Medicine. 2012. De Santis M et al. Arch of IntMedicine, 2002. Source: Antiretroviral Pregnancy Registry Steering Committee http://www.APRegistry.com Siberry GK et al. AIDS, 2012
2013 Consolidated ARV Guidelines Treatment Recommendations for Pregnant and Breastfeeding Women: Critical Issues HIV/AIDS DEPARTMENT
Evolution of WHO PMTCT ARV Recommendations Launch July 2013 2010 2001 2004 2006 Move towards: more effective ARV drugs, extending coverage throughout MTCT risk period, and ART for the mother’s health
Rationale • Limited coverage and implementation of PMTCT and ART for pregnant women in many high burden countries • ~ 1.4 million HIV+ pregnant women • 65% PMTCT ARV coverage • Limited ART in those eligible for treatment • High loss to follow-up along PMTCT cascade • Low ARV coverage during breastfeeding Steady progress reducing infant infections • Complexity of Option A • Different treatment and prophylaxis regimens through pregnancy and breastfeeding • Difficulty of long-term NVP dosing for infants • Requirement for CD4 to determine eligibility • Follow up along the PMTCT cascade is very low • Current approach needs to be optimized to achieve universal access and elimination 600 500 400 300 200 100 0 • 2009: ~430,000 infant infections • 2012: ~290,000 infant infections • 2015: Global Plan target <40,000
Recommendations “Option B+” “Option B” • All pregnant and breastfeeding women infected with HIV should initiate triple ARVs (ART), which should be maintained at least for the duration of mother-to-child transmission risk. Women meeting treatment eligibility criteria should continue lifelong ART . • (strong recommendation, moderate-quality evidence) • For programmatic and operational reasons, particularly in generalized epidemics, all pregnant and breastfeeding women infected with HIV should initiate ART as lifelong treatment. • (conditional recommendation, low-quality evidence) • In some countries, for women who are not eligible for ART for their own health, consideration can be given to stopping the ARV regimen after the period of mother-to-child transmission risk has ceased. • (conditional recommendation, low-quality evidence)
Rationale: Shift from Option A to B+ or B • Major issue now is not “when to start” or “what to start” but “whether to stop”
Programmatic considerations for B+ • Initiate all HIV+ pregnant and breastfeeding women on ART • Operational and programmatic advantages to lifelong ART for pregnant and breastfeeding women (“B+”), particularly in settings with: • Generalized epidemics • High fertility (though need to strengthen FP) • Long duration of breastfeeding • Limited access to CD4 to determine ART eligibility • High partner serodiscordance rates • National programmes need to decide B or B+
Implementation Issues Adequate planning for changes in guidelines Expansion and integration of ART into PMTCT sites Supply chain for ARVs (avoidance of stock-outs) Task-shifting for ART initiation Adherence, retention, follow up, linkages with chronic ART All MNCH sites become ART sites Access to ART monitoring • Major challenge for PMTCT and MNCH settings: • How to expand access to VL monitoring? • How to utilize CD4 data, especially for women with high baseline CD4?
Summary of changes to recommendations: What ART to Switch to