Download
1 / 87
880 likes | 926 Views
Learn the basics of cardiac dysrhythmia interpretation, including the cardiac cycle, autonomic nervous system, and electrophysiologic properties. Explore major electrolytes affecting cardiac function and the movement of ions within cardiac cells.

E N D
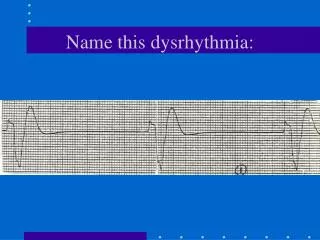
Basic Dysrhythmia Interpretation NURS 108 Spring 2008 Majuvy L. Sulse RN, MSN,CCRN
Cardiac Cycle • Systole-simultaneous contraction of ventricles, lasts 0.28 sec • Diastole- ventricular relaxation, lasts 0.52 sec • One cardiac cycle occurs every 0.8 sec
Cardiac Cycle • Stroke volume-volume of blood (70cc) pumped out of one ventricle of the heart in a single contraction • Heart rate- number of contractions per minute(60-100bpm • Cardiac output-amount of blood pumped by the left ventricle in 1 minute (4-8L/min) • CO= SV XHR
Cardiac Cycle • Preload-degree of myocardial fiber stretch at the end of diastole • Afterload-resistance against which the heart must pump to eject blood through the semilunar valves and into peripheral vessels • STARLING’S Law-the more the muscle fibers are stretched up to a certain point, the more forceful the subsequent contraction will be. • Systemic vascular resistance (impedance)- amount of opposition to blood flow offered by the arterioles, pressure the heart must overcome to open the aortic valve
Autonomic Nervous System • Sympathetic-prepares for physical activity-fight or flight response-norepinephrine (Adrenergic nerve endings) • Alpha-vasoconstriction • Beta • Beta 1-increase HR & contractility • Beta 2-bronchial dilation & vasodilation • Parasympathetic-rest & digest function • Acetylcholine (cholinergic nerve endings)
Electrophysiologic Properties • Automaticity-ability to generate an electrical impulse spontaneously & repetitively • Excitability-ability to be electrically stimulated or respond to an electrical stimulus • Conductivity-ability to receive an electrical stimulus and transmit to other cardiac cells • Contractility-also rhythmicity is the ability to shorten and cause contraction in response to an electrical stimulus-coordination of contraction to produce a regular heartbeat
Major electrolytes that affect Cardiac Function • 3 major cations • K-performs a major function in cardiac depolarization and repolarization • Sodium plays a vital part in myocardial depolarization • Calcium is important in myocardial depolarization and contraction. • Magnesium-acts as transporter for Na & K across cellular membranes. Also plays an important function in muscular contraction
Movement of Ions • Resting cardiac cells (Polarization) –inside the cell is negatively charged. K is greater in the cell; Na greater outside the cell (positively charged)-Resting membrane potential • Depolarization (action Potential)-sodium-potassium exchanged pump resulting in positive polarity inside the cell membrane. Myocardial contraction occurs. • Repolarization-recovery or resting phase; positive charges are again on the outside and negative charges in the inside
Refractory Periods • Ensures that the muscle is totally relaxed before another action potential occurs • Atrial muscle-0.15 sec • Ventricular muscle-.25-.30 sec
Refractory Periods Absolute refractory period-cardiac muscle cannot be depolarized. Corresponds to beginning of QRS to peak of T wave Relative refractory period-cardiac muscles stimulated to contract prematurely if stimulus is stronger than normal. Corresponds with down slope of T wave
Electrical Conduction Pathway • SA node (60-100bpm) • Internodal pathways • AV node ( 40-60bpm) • Bundle of His • Bundle Branches • Purkenje networks (20-40bpm)
EKG • ECG/EKG-a graphic representation of cardiac activity • 12 lead-shows electrical activity from 12 different planes of the heart-used as a diagnostic tool rather than a monitoring device • Electrode-adhesive pad that contains conductive gel and designed to be attached to skin • Leads-wires generally color coded. For the EKG to receive a clear picture of electrical impulses, there must be a positive, a negative and a ground. The exact portion of the heart being visualized depends on lead placement
EKG Leads • Baseline-isoelectric line-no current flow in the heart; consists of positive, negative deflections or biphasic complex • 3 or 5 lead- used for monitoring the current cardiac activity of patients at risk for cardiac abnormalities • Lead ll or MCL1-modified chest leads mostly used because of ability to visualize P waves. MCL provides a R sided view of the heart. MCL6-L sided view of the heart
EKG Leads • Limb leads • Bipolar leads-measures activity between 2 points (I, II, III) • Unipolar leads-positive electrodes only-aVR, aVL, aVF • Chest leads-6 precordial leads
Segments and Intervals • P wave-deflection representing atrial depolarization • PR segment-isoelectric line from end of P wave to beginning of QRS-impulse is traveling through the AV node. PR interval-0.12-0.20(time for atrial depolarization-AV node-Purkenje fibers) • QRS complex-ventricular depolarization. QRS duration of 0.04-.10 sec from QRS to J-point • ST segment-early ventricular repolarization from J-point to beginning of T wave. Elevations not more than 1 mm or deflections o.5 mm from isoelectric line • T wave- ventricular repolarization, usually rounded, positive deflection • U wave-smaller polarity as T wave-slow repolarization- not normally seen except in hypokalemia • QT interval-total time for ventricular depolarization and repolarization
HR Determination • 6 second method • count QRS complexes in a 6 sec strip x 10 (30 large boxes in 6 sec strip) • P-P or R-R interval method • count number of small blocks in a P- P or R-R interval and divide into 1500 (no. of small blocks in 1 min) • Count the number of large blocks in an interval and divide into 300 (number of large blocks in 1 minute) • Memory method
ECG Rhythm Analysis • Analyze P waves- P wave is present. shape is consistent, must be before each QRS • Analyze QRS complex- QRS complex is present & consistent • Determine atrial rhythm or regularity- check regularity by assessing P-P or R-R • Determine ventricular rhythm or regularity-check regularity by assessing R-R • Determine heart rate-use one of the methods • Measure the PR interval-measurement should be constant and should be between 0.12-0.20 • Measure the QRS duration-measurement should be constant and should be between 0.04-0.10 sec • Interpret the rhythm
General Rules • First & most important, LOOK at your PATIENT! • Read every strip from left to right • Apply the systematic approach • Avoid shortcuts and assumptions. • Ask and answer each question in the ECG analysis approach
Artifacts • Waveforms outside the heart-interference caused by: • Patient movement wandering baseline • Loose or defective electrodes-lost contact with patient’s skin • Improper grounding-in touch with an outside source of electricity • Faulty EKG apparatus Patient assessment is critical
Normal Sinus Rhythm SA node generated an impulse that followed a normal pathway, the heart rate falls within the range, atrial & ventricular rhythms are regular, P waves preceded every QRS and QRS is within 0.12sec
Sinus Bradycardia SA node fires slower than normal heart rate-less than 60bpm Rhythm is regular P wave upright and same shape PR is constant .12-.20sec QRS-normal <.12sec
Sinus Bradycardia • Causes: • Vagal stimulation, MI, hypoxia • Digitalis toxicity • Medication side effects • Normal to athletes • Adverse effects: • Dizziness, weakness, syncope, diaphoresis, pallor, hypotension • Treatment • According to symptoms, atropine to speed up heart rate, pacemaker
Sinus Tachycardia SA node fires at a rate faster than normal but conduction pathway is normal. All criteria for interpretation are the same except that the heart rate is faster.
Sinus Tachycardia • Causes • Emotionally upset, pain, fever, thyrotoxicosis, hypoxia, hypovolemia, inhibition of vagus nerve, • Caffeine, norepinephrine, theophylline • Adverse effects • Angina, dizziness, hypotension, increased in cardiac workload • Treatment • Treat the cause • Medications may be given- betablockers
Sinus Arrhythmia • The only irregular rhythm from the sinus node and has a cyclic pattern that usually corresponds with breathing • Rate- varies with respiratory pattern • Regularity-irregular in a repetitive pattern • P waves-Upright in most leads, same shape and one to each QRS P-P interval is irregular • QRS-<.12 sec • Cause-usually caused by breathing pattern but can also heart disease • Treatment- usually non required
Atrial Dysrhythmias • SA node fails to generate an impulse • Atrial nodes or internodal pathways may initiate an impulse and follows the conduction pathway • Dysrhythmias of this type are not lethal • Accessory pathway-irregular muscle connection between atria and ventricles that bypasses the AV node
Premature Atrial Contractions • Causes- atria becomes hyper and fire early caused by medications, caffeine, tobacco, hypoxia or heart disease • Adverse effects-if frequent can be a sign of impending heart failure or atrial tachycardia or fibrillation • Treatment-O2, omit caffeine, tobacco or other stimulants. Give digitalis or quinidine, treat heart failure.
Premature Atrial Contractions Rate normal Rhythm usually regular except for a PAC P waves shaped differently from a normal P wave or hidden in preceding T wave PR interval .12 to .20sec QRS .12sec similar to underlying rhythm
Supraventricular Tachycardia (SVT) • Tachycardia (>150 bpm) originating above the ventricles-SA node, atria, AV nodes • P waves not discernible-hidden in T waves • Paroxysmal-starts & ends abruptly • Causes-same as PAcs • Adverse effects- palpitations, light-headedness, dizziness, shortness of breath, chest pain, fainting =decreased cardiac output • Treatment-vagal maneuvers (cough, bear down), carotid massage, or medications digitalis, calcium channel blockers, beta blockers, Adenosine
Supraventricular Tachycardia (SVT) Rate 150-250bpm Rhythm regular P waves not discernible PR not discernible QRS usually less than .10sec
Atrial Flutter • Results when one irritable atrial foci fires out regular impulses at a rapid rate that P waves are in a sawtooth pattern • Av node (gatekeepers) cannot depolarize fast enough to keep up, many impulses never get through to ventricles. Conduction ratio is variable-2:1block, 3:1 block or 4:1 block. Slow ventricular response-VR of <60pm; rapid VR >100-150bpm) • Causes-acute MI, CHF, digitalis toxicity, pulmonary embolism, SA node disease, septal defects • Adverse effects-decreased cardiac output • Treatment-digitalis, cardioversion, calcium channel blockers, ablation
Atrial Flutter Rate atrial 250-300bpm, ventricles-variable Rhythm regular if conduction ratio is constant, irregular if conduction rate varies P waves replaced by fluttery waves PRnot measurable QRS <.12sec
Atrial Fibrillation • Most common atrial dysrhythmia in elderly patients • Multiple atrial impulses from different locations all at the same time (350-600bpm) • Ventricular response maybe rapid (100-150bpm) or slow (< 60bpm) • Causes-maybe chronic MI CHF, valvular heart disease, hyperthyroidism • Adverse effects-decreased cardiac output, blood clots which can cause MI, stroke or clot in the lung • Treatment- Digitalis, quinidine, cardizem, anticoagulant as coumadin, cardioversion
Junctional Rhythms • Arrhythmia originating in AV node • HR= 40-60bpm; accelerated =60-100bpm; junctional= 100-140bpm • P wave-absent, inverted before or after a QRS • PR interval-<.12if P precedes a QRS • QRS <.12sec • Cause-vagal stimulation, hypoxia, ischemia of SA node, MI, digitalis toxicity • Treatment-varies according to type of arrhythmia. Atropine to increase HR, withhold or decrease medication that can slow heart rate
Ventricular Dysrhythmias • Ventricles serves as pacemaker • Heart rate significantly reduced (20-40 beats per min • Normal conduction system bypassed • QRS bizarre in appearance & >0.12 sec • P waves absent (buried or hidden in QRS) • Rhythms considered life threatening
Premature Ventricular Complexes (PVCs) • A single ectopic (out of place) complex from an irritable site • Indicates increased myocardial irritability • Precursors of more serious lethal rhythms • Cardiac output compromised • Causes • Myocardial ischemia, Emotional stress, increased physical exertion, CHF, electrolyte imbalance, digitalis toxicity or acid base imbalances • Treatment- based on symptoms and causative factors • O2 and antidysrhythmics
PVCs • Unifocal-arise from one single site • Multifocal- originate from different sites • Ventricular bigeminy- every other beat is a PVC • Ventricular trigeminy-every third beat is a PVC • Ventricular quadrigeminy- every 4th beat is a PVC • Interpolated- a PVC between two sinus beats • Couplet or repititive PVCs- two PVCs occurring together without a normal complex in between • Salvos-3 or more PVCs in a row (Vtach)
Premature Ventricular Contraction (PVC) Unifocal PVCs Multifocal PVCs