Download
1 / 21
250 likes | 507 Views
ATOPIC DISEASE. D. pteronyssinus. ATOPIC DISEASE. Atopic dermatitis. Aller g ic IgE mediated asthma. IgE mediated rhinitis. Food allergy IgE mediated. Cause & hypothesis of ATOPIC DISEASE. hygiene. Genetic hypothesis Hygiene hypothesis Shift from Th1 to Th2

E N D
D. pteronyssinus ATOPIC DISEASE Atopicdermatitis AllergicIgEmediated asthma IgEmediated rhinitis FoodallergyIgEmediated
Cause & hypothesis of ATOPIC DISEASE hygiene • Genetichypothesis • Hygiene hypothesis • Shift from Th1 to Th2 • Decreased number/activity of regulatory T cells • Changes in indoor air quality • Changes in life style
Systemic Model for AtopyDisease • Systemicallergicinflammationconveysthe concept that allergy is a systemicimmunologicdysfunctionwithlocalmanifestations
TheHygieneHypothesis • Improvedhygieneinindustrializedsocieties - Improved public health - Use of vaccines and antibiotics • Decreased infections that normally stimulate the immune system to work against asthma. • The following have a decreased risk ofasthma: - biggerfamilies - earlyplacementinday-care - exposure to farm animals and products- exposure to bacterialendotoxins - limited use of antibiotics
TheAtopicMarch • “Atopicmarch” 1.Atopic dermatitis (±foodallergy) – 2/3.inhalant allergy - allergicrhinitis -3/2. asthma •Food Allergy (0 – 1 year old) • Eczema (3 months – 2-3 years old) • Allergic Rhinitis (2 years – adulthood) • Asthma (3 years – adulthood)
“AtopicMarch” Incidence 0 5 10 15 Age (years)
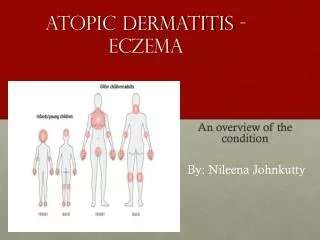
AtopicEczema & AllergyDermatitis • Distribution of the rash typically varies with age: 1) In infancy (3 months to 2 years) the cheeks, wrists and extensoraspects of the arms and legs are usually involved.The entire body may be affected but the nappy area is usually spared. 2) In young children (2 years to 12 years) flexor surfaces, the neck, wristsand ankles are generally involved. 3) In teenagers and young adults flexural surfaces, the face(especially periorbital region), hands and feet are frequentlyaffected.
Association Between AD and Asthma Bergmann (1998, clinexpallergy) - prospective birth cohort study, n= 1314, 5 y - if AD at months 3 and one parent/sibling atopic: -> 50%chance of asthma at age of 5-6 Castro-Rodriguez (1999, AJRCCM) - longitudinal, retrospective study, n = 986 - if AD and parental asthma: -> 75% chance of asthmaduringschoolyears Leung (JACI 2000) - if AD before age of 5: -> 80% chance to develop asthmaorallergicrhinitis.
AllergicRhinitis and Asthma: • TwoRelatedConditions • Linked by One Common Airway
Risk • Asthmain 40% of AR patients • Rhinitis in 75%- 80% of asthmatics • Rhinitis increases risk of asthma 3-fold “One airway” hypothesis • Nasal and lung pathology is similar • Nasal allergen challenge lower airwayinflammation
Asthma HISTORY • Past / Family History of atopy (allergy) esp. rhinitis(hay fever), conjunctivitis, eczema or urticaria may point to asthma • History of childhood asthma important (but not all asthma begins in childhood - some present for the first time in adult life and these patients tend not to be allergic)
Pathogenesis of asthma Type I hypersensitivity Type IV hypersensitivity “remodeling” H. HogenEsch, 2009
Allergy and Asthma are manifestations of complex and dynamic networks Environmental component Genetic component Allergen exposures Lifestyle Medications etc… SNPs, etc. Genes and pathways Cell, immune, and inflammatory phenotypes, etc. Bronchoconstriction, Mucus Secretion, Hyperreactivity, IgE levels, Airway Structure
Risk factors and phenotypes vary over time H E A L T H O U T C O M E S M A C R O S O C I A L E N V T E N V I R O N M E N T M I C R O S O C I A L S U B C L I N I C A L LIFE COURSE PERSPECTIVE C L I N I C A L Psycho-neuro-endocrine cascades Psycho-neuro-immune cascades (Physiological Reactions)
Pathogenesis of ChildhoodAsthma • Sensitization • Foodallergy • Eczema • AllergicRhinitis • RecurrentWheezing +Genetics+Environment +Age+ Allergens →Asthma
Food Allergies: 90% accounted for by 5 foods • 5 most common allergens in infants•Cow Milk•Soy•Wheat•Peanuts/Tree nuts•Egg Cowmilk protein: • •the most common food antigen in infants
But …. • > 50% of children who develop allergy do not have a family history
On thebegininig….. AD TheEnd...