Download

1 / 43
430 likes | 459 Views
Delve into the fascinating world of the thalamus, the central hub for processing sensory information in the brain. Learn about its anatomy, major nuclei, functions, and clinical correlations.

E N D
The Thalamus is a Scanner . All information comes into the thalamus before being distributed to other parts of the brain. It’s sometimes called the scanner because it constantly scans the environment for information
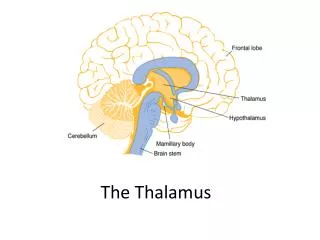
Introduction- The Thalamus ventral view Dorsal view
The Thalamus (from Greek = bedroom, chamber) • 3.5cm in length, • 1.5cm in width • 80 % of the diencephalon • paired and symmetric part of the brain • There are 2 thalami, • one on each side of the 3rd ventricle, they are connected by the interthalamic adhesion
Introduction- The Thalamus Insula Internal capsule Lentiform nucleus Coronal Section
Thalamus Dorsal View
Boundaries of the Thalamus • Anterior: • interventricular foramen • Posterior: • free pole of the pulvinar • Dorsal: • free surface underlying the fornix and the lateral ventricle • Ventral: • plane connecting the hypothalamic sulci
Boundaries of the Thalamus Medial: third ventricle Lateral: posterior limb of the internal capsule Thalamus
Relations Dorsal: lateral ventricle Anterior: interventricular foramen Medial: 3rd ventricle Lateral: Internal capsule Ventral: Subthalamus & Hypothalamus Caudal: midbrain
Anatomic Divisions Internal medullary lamina Thin sheet of myelinated fibers Divides the thalamus into three major divisions, each containing specific nuclei: Anterior Medial Lateral Not included in these divisions are The intralaminar nuclei The Reticular nucleus
Anatomical Divisions Anterior Division Anterior nucleus Medial Division Dorsomedial Nucleus (DM) Lateral Division Dorsal Tier Lateral dorsal (LD) Lateral Posterior (LP) Pulvinar Ventral Tier Ventral Anterior (VA) Ventral Lateral (VL) Ventral Posterior (VP) Ventral posteriolateral (VPL) Ventral posteriomedial (VPM) Ventral posterioinferior
DORSAL ANT. POST. VENTRAL
Internal medullary lamina Interthalamic adhesion Ant. Nucleus Medial nucleus Posterior LD Anterior V A LP V L Pulvinar VPL VPM MGB LGB .
Functional subdivision According to function, the thalamus may be divided into three groups 1. Nonspecific relay nuclei 2. Association nuclei :DM,LD,LP & Pulvinar 3. Specific relay nuclei :MGB, LGB, VPL, VPM, VL VA,
Main Thalamic Nuclei and Their Major Connections Anterior part • Contains the anterior thalamic nucleus • This nucleus receives hypothalamic input from the mammillary nucleus via the mamillothalamic tract • It receives hippocampal input via the • fornix (hippocampus). • It projects to the cingulate gyrus. • Function :associated with that of the limbic system and is concerned with emotional toneand the mechanisms of recent memory
Main Thalamic Nuclei and Their Major Connections Lateral part • ventral anterior & ventral lateral nuclei • Motor relay nuclei associated with somatic motor system • VA receives from globus pallidus & S.nigra. Projects to supplementary motor area (6). • VLreceives from cerebellar nuclei ( Dentate) & globus pallidus. Projects to primary (4) & supplementary (6) motor cortex.
Main Thalamic Nuclei and Their Major Connections Lateral part • VL circuits: • Cerebral-cerbellar-cerebral • Cerebral-basal ganglia-cerebral • VL lesionswould ameliorate contralateral tremor & rigidity in patients of Parkinson's disease
Main Thalamic Nuclei and Their Major Connections Medial part • Contains the large Mediodorsal nucleusand several smaller nuclei • The Mediodorsal nucleusis reciprocally connected to the • Prefrontal cortex of the frontal lobe. • It has abundant connections with all other groups of thalamic nuclei • It receives input from • amygdaloid nucleus, • temporal neocortex, and • substantia nigra.
Main Thalamic Nuclei and Their Major Connections Medial part • Function: • integration of a large variety of sensory information, including somatic, visceral, and olfactory information • relate this information to one’s emotional feeling
Main Thalamic Nuclei and Their Major Connections Mediodorsal nucleus (dorsomedial nucleus) Clinical correlate • When destroyed, the result is a memory loss • (Wernicke-Korsakoff syndrome). • It plays a role in the expression of affect, emotion, and behaviour (limbic function).
VP Main Thalamic Nuclei and Their Major Connections Lateral part – Ventral tier • Theventral posterior nucleus • Recieves • general somatic afferent (GSA; pain and temperature) and • special visceral afferent (SVA; taste) pathways. • Contains three subnuclei
VPL Main Thalamic Nuclei and Their Major Connections Lateral part – Ventral tier Ventral posterolateral (VPL) nucleus • Receives the spinothalamic tracts and the medial lemniscus (tactile discrimination, vibration, form recognition, joint and muscle sensation, proprioception). • Projects to thesomatosensory cortex (postcentral gyrus - areas 3, 1, and 2). • These projections pass through the post. Limb of the internalcapsule and corona radiata • Lesion results in contralateral loss of pain and temperature sensation, and loss of tactile discriminationin the trunk and extremities
VPM Main Thalamic Nuclei and Their Major Connections Lateral part – Ventral tier Ventral posteromedial (VPM) nucleus • Receives the trigeminothalamictracts. • Receives the taste pathwayvia the solitary nucleus and the parabrachial nucleus. • Projects to the somatosensory cortex(areas 3, 1, and 2). • These projections pass through the post. Limb of the internalcapsule and corona radiata • Lesion results in contralateral loss of pain and temperature sensation, and loss of tactile discrimination in the head; results inipsilateralloss of taste.
Main Thalamic Nuclei and Their Major Connections Lateral part – Ventral tier Ventral posteroinferior (VPI) nucleus • Receives vestibulothalamic fibres from the vestibular nuclei. • Projects to thevestibular area of the somatosensory cortex. VPI
Main Thalamic Nuclei and Their Major Connections Intralaminar nuclei • A groups of nuclei embedded within the internal medullary lamina • input from the brainstem reticular formation,and other thalamic nuclei, spinothalamic and trigeminothalamic tracts • efferent fibres to other thalamic nuclei which, in turn, project diffusely to theentire neocortex. • The nuclei are believed to influence thelevels of consciousnessand alertnessin an individual – the level of activity of cerebral cortex
A A MD VA VL VPL P VPM LGB MGB
Blood Supply of the Thalamus 1.Posterior communicating artery • Gives rise to the • anterior thalamoperforating arteries
Blood Supply of the Thalamus 2.Posterior cerebral artery • Gives rise to: • posterior choroidal arteries. • posterior thalamoperforating arteries.
Thalamogeniculate artery Thalamoperforating artery
Function of the Thalamus • Following removal of the cortex the thalamus can appreciate crude sensation. • However, the cerebral cortex is required for the interpretation of sensation based on past experience.
Functional Roles Thalamus has four basic functional roles: Sensory All sensory information (except olfaction) is relayed to the cortex via the thalamus Motor Motor system outputs from the basal ganglia and cerebellum are relayed by the thalamus Emotion/memory The thalamus is part of the Papez circuit and helps control some emotional and memory information going to limbic cortex (cingulate gyrus) Vegetative The thalamus has some intrinsic nuclei associated with alertness and arousal. Can be associated with disorders of consciousness
Functional Roles Thalamus doesn’t just send information to the cortex. It receives cortical feedback This signal helps regulate what is coming to the cortex Cortical input is a feedback inhibition loop, letting the thalamus know that information has been received and inhibiting further relaying of the information
Thalamic Function • Gateway to the cerebral cortex • Sorts, edits, and relays information • Afferent impulses from all senses and all parts of the body • Impulses from the hypothalamus for regulation of emotion and visceral function • Impulses from the cerebellum and basal nuclei to help direct the motor cortices • Mediates sensation, motor activities, cortical arousal, learning, and memory
Clinical considerations Thalamic syndrome (Dejerine and Roussy) • Is usually caused by occlusion of aposterior thalamoperforating artery! • Classic signs are: • Contralateral hemiparesis • Contralateral hemianesthesia • Elevated pain threshold • Spontaneous, agonizing, and burning pain (hyperpathia, Thalamic Pain Syndrome) • Athetotic posturing of the hand (thalamic hand).
Thalamic syndrome of Dejerine-Roussy • Stroke caused by occlusion of a branch of the PCA supplying the posterior and lateral thalamic nuclei. • Initially there is a contralateral hemisensory loss in the head and body. • Followed by dysesthesia (disagreeable sensation produced by ordinary stimuli), spontaneous intractable pain (thalamic pain) and emotional instability. (axial CT scan) Joseph Jules Dejerine 1849-1917 Gustave Roussy 1874-1948
This syndrome may include: 1.Spontaneous pain & 2.Evidence of emotional instability such as unprovoked laughing and crying