Download
1 / 23
230 likes | 246 Views
Neurologic Emergencies: vestibular events. Todd M. Bishop, DVM, DACVIM (Neurology) Thursday February 6 th , 2014. Goals of this mini-lecture. Recognize the clinical signs Correlate with the neurologic exam Perform point-of-care diagnostic testing Provide initial therapeutic intervention(s)

E N D
Neurologic Emergencies: vestibular events Todd M. Bishop, DVM, DACVIM (Neurology) Thursday February 6th, 2014
Goals of this mini-lecture • Recognize the clinical signs • Correlate with the neurologic exam • Perform point-of-care diagnostic testing • Provide initial therapeutic intervention(s) • Know when to discuss referral * Making anatomic and differential diagnoses will NOT be emphasized in this talk but the details are in the notes.
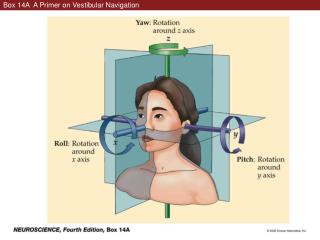
What the client sees … • Head tilt • Balance loss; walking as if “drunk” • Jerking eye movements • Eyeball deviation • Nausea, vomiting, drooling • Wide-based stance • Inability to stand • Listing, leaning, falling to one direction • Rolling to one side (“alligator rolling”)
What you should look for … • Mentation change • Cranial nerves abnormalities • Strabismus, nystagmus • Gait and Posture alteration • Head tilt, ataxia • Posturalreactions deficits • Delayed hopping and placing www.rawstory.com
The quick and dirty • When is it in the brain (central vestibular)? • Mentally inappropriate • Vertical nystagmus • Changing direction nystagmus • Right to left • Vertical to horizontal • but NOT horizontal to rotary to the same side! • Postural reaction deficits
Etiologies* PERIPHERAL • Idiopathic • Otitis M/I • Hypothyroidism • Ototoxicity • Trauma • Neoplasia CENTRAL • Metabolic • Malformative • Inflammatory • Infectious • Infarction (vascular) • Neoplastic • Degenerative * Remember this is NOT the emphasis of this lecture!
Diagnostic testing • Primary Care • CBC/Chem/UA/CXR/BP • Thyroid panel • Otoscopic exam • Cytology and culture • Myringotomy • Sedated skull radiographs • Referral • MRI > CT scan • CSF tap
Basic Medical Work-up • CBC/Chem/T4/UA • Thoracic radiographs • A BLOOD PRESSURE
Soapbox ALERT ! • I can not emphasize the importance of the basic medical work-up enough ! • You may find the cause or a complicating disease process !! • This MUST be done before advanced testing can be considered !!! • People … it makes financial sense !!!! • with one exception … same day referral marvimarti.com
Thyroid testing • A simple total T4 will suffice for cats • Dogs need a complete thyroid panel HYPERT4→high BP→stroke→vestibular signs hypoT4→atherosclerosis→stroke→vestibular signs hypoT4→abN metabolism in VIII→vestibular signs
Otoscopic exam http://www.petearclinic.com/images_video.htm
External ear cytology & culture http://leicesterskinvet.com/wp-content/uploads/2010/10/Malassezia-pachydermatis.jpg
Myringotomy (tympanocentesis) http://www.welchallyn.com/apps/products http://glomed.biz/products.php?sub_id=40 http://www.rush.edu/webapps/rml/RMLTestEntryDtl.jsp?id=3264 http://www.neuralstainkit.com/Laboratory_Supplies.php
Sedated skull radiographs Textbook of Veterinary Diagnostic Radiology- Thrall
Empiric therapies * • IV fluids • Antibiotics • Dimenhydrinate (Dramamine) • Meclizine (Bonine, Antivert) • Cerenia • Benzodiazepines • Corticosteroids? * Regardless of etiology!
Intravenous Fluids • Rehydrate after vomiting • Maintain vascular volume (anorexia) • Combat ongoing losses (drooling) • Promote cerebral profusion (especially important in ischemic cerebrovascular disease)
Antibiotic therapy • Common otic flora • Strep, Staph, Malassezia • Base treatment on cytology and culture • Empiric treatment options: • Cephalosporin • Amoxicillin • Fluoroquinolone • Fluconazole
Dimenhydrinate • Antihistaminic (H1), antiemetic and anticholinergic effects • Acetylcholine stimulation of the vestibular and reticular systems may be blocked • 4-8 mg/kg PO SID-TID • 12.5 mg PO SID-TID (cat) • 25–50 mg PO SID-TID (dog) essex1.com
Meclizine • Antihistamine with sedative & antiemetic effects • H1 receptor blocker • 25 mg / dog PO SID x 3-4 days • 12.5 mg / cat insightpharma.com
Cerenia • Maropitant (mar-oh-pit-ent) Citrate • Neurokinin (NK1) Receptor Antagonist • Inhibits Substance P a neurotransmitter involved in vomiting • Acts at the vomiting center to treat motion sickness • 8 mg/kg PO q 24h for up to 2 consecutive days vinoenpaso.at
Benzodiazepines • Diazepam or Midazolam : • 0.5 mg/kg IV bolus • 0.5 mg/kg/hr IV CRI over 24-72 hrs • Sedative effect • Inhibitory neurotransmitter in the vestibular system • Metronidazole toxicosis antidote bipolarblast.wordpress.com
Corticosteroids • Should ideally be employed only after a definitive diagnosis has been made • Can be added if all other empiric therapies are failing and clients not interested in referral • If using empirically consider an anti-inflammatory dose (ie. Prednisone 0.5 mg/kg BID)
When to refer a case? • After a patient is stabilized • Once preliminary testing is done • When there is no response to general supportive care described above • When central disease is suspected