Download
1 / 34
340 likes | 348 Views
Outbreak investigation, response and control. IDSP training module for state and district surveillance officers Module 8. Learning objectives (1/3). Define an outbreak/epidemic List the various ways of detecting an outbreak/ epidemic

E N D
Outbreak investigation, response and control IDSP training module for state and district surveillance officers Module 8
Learning objectives (1/3) • Define an outbreak/epidemic • List the various ways of detecting an outbreak/ epidemic • List the modes of transmission of causative agents of outbreaks • Describe warning signs of an impending outbreak
Learning objectives (2/3) • Specify the operational threshold levels of diseases under surveillance for outbreak investigations • List the members of rapid response team in your district • Enumerate the situations when DEIT would be initiated • Describe the steps of epidemic investigation to establish an outbreak and determine its etiology
Learning objectives (3/3) • Outline the appropriate control measures to be taken when the nature of the outbreak is established: • Water borne diseases • Vector borne diseases • Vaccine preventable disease outbreaks • Outbreaks of unknown etiology
Definition of an outbreak • Occurrence in a community of cases of an illness clearly in excess of expected numbers • The occurrence of two or more epidemiologically linked cases of a disease of outbreak potential constitutes an outbreak • (e.g., Measles, Cholera, Dengue, Japanese encephalitis, or plague)
Outbreak and epidemic: A question of scale • Outbreaks • Outbreaks are usually limited to a small area • Outbreaks are usually within one district or few blocks • Epidemics • An epidemic covers larger geographic areas • Epidemics usually linked to control measures on a district/state wide basis • Use a word or the other according to whether you want to generate or deflect attention
Endemic versus epidemic • Endemicity • Disease occurring in a population regularly at a usual level • Tuberculosis, Malaria • Epidemics • Unusual occurrence of the disease clearly in excess of its normal expectation • In a geographical location • At a given point of time
Sources of information to detect outbreaks • Rumour register • To be kept in standardized format in each institution • Rumours need to be investigated • Community informants • Private and public sector • Media • Important source of information, not to neglect • Review of routine data • Triggers
Early warning signals for an outbreak • Clustering of cases or deaths • Increases in cases or deaths • Single case of disease of epidemic potential • Acute febrile illness of an unknown etiology • Two or more linked cases of meningitis, measles • Unusual isolate • Shifting in age distribution of cases • High vector density • Natural disasters
Verify Recognize the magnitude Diagnose the agent Identify the source and mode of transmission Formulate prevention and control measures Host Environment Agent An outbreak comes from a change in the way the host, the environment and the agent interact: This interaction needs to be understood to propose recommendations Objectives of an outbreak investigation
Outbreak preparedness: A summary of preparatory action • Formation of rapid response team • Training of the rapid response team • Regular review of the data • Identification of ‘outbreak seasons’ • Identification of‘outbreak regions’ • Provision of necessary drugs and materials • Identification and strengthening appropriate laboratories • Designation of vehicles for outbreak investigation • Establishment of communication channels in working conditions (e.g., Telephone)
Basic responses to triggers • There are triggers for each condition under surveillance • Various trigger levels may lead to local or broader response • Tables in the operation manual propose standardized actions to take following various triggers • Investigations are needed in addition to standardized actions
Importance of timely action: The first information report (Form C) • Filled by the reporting unit • Submitted to the District Surveillance Officer as soon as the suspected outbreak is verified • Sent by the fastest route of information available • Telephone • Fax • E-mail
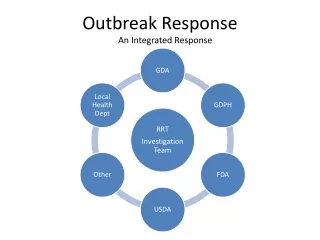
The rapid response team • Composition • Epidemiologist, clinician and microbiologist • Gathered on ad hoc basis when needed • Role • Confirm and investigate outbreaks • Responsibility • Assist in the investigation and response • Primary responsibility rests with local health staff
The balance between investigation and control while responding to an outbreak
Steps in outbreak response • Verifying the outbreak • Sending the rapid response team • Monitoring the situation • Declaring the outbreak over • Reviewing the final report
Step 1: Verifying the outbreak • Identify validity of source of information to avoid false alarm/a data entry error • Check with the concerned medical officer: • Abnormal increase in the number of cases • Clustering of cases • Epidemiological link between cases • Occurrence of some triggering event • Occurrence of deaths
Step 2: Sending the rapid response team • Review if the source and mode of transmission are known • If not, constitute team with: • Medical officer • Epidemiologist • Laboratory specialist • Formulation of hypothesis on basis of the description by time, place and person • Does the hypothesis fits the fact • YES: Propose control measures • NO: Conduct special studies
Time Acute hepatitis by week of onset in 3 villages, Bhimtal block, Uttaranchal, India, July 2005 90 Outlying case-patient might have been a source 80 70 60 50 Number of cases 40 30 20 10 0 1st week 3rd week 1st week 1st week 1st week 1st week 3rd week 3rd week 3rd week 4th week 4th week 4th week 2nd week 4th week 2nd week 2nd week 2nd week May June July August September Week of onset
Suspected spring Place Incidence of acute hepatitis by source of water supply, Bhimtal block, Uttaranchal, India, July 2005 Water supply Spring Reservoir Pipeline Attack rate < 5% 5-9% 10% + Dov Mehragaon main village Mehragaon Hydle colony Mehragaon Chauriagaon
Person Incidence of acute hepatitis by age and sex in 3 villages, Bhimtal block, Uttaranchal, India, July 2005
When to ask for assistance from the state level? • Unusual outbreak • High case fatality ratio • Unknown etiology • Trigger level three and above
Steps of a full outbreak investigation using analytical epidemiology to identify the source of infection • Determine the existence of an outbreak • Confirm the diagnosis • Define a case • Search for cases • Generate hypotheses using descriptive findings • Test hypotheses based upon an analytical study • Draw conclusions • Compare the hypothesis with established facts • Communicate findings • Execute prevention measures Requires assistance from qualified field epidemiologist (FETP)
Cohort to estimate the risk of hepatitis by water supply, Mehragaon village, Uttaranchal, India, July 2005 Analytical epidemiology compares cases and non cases or exposed versus unexposed to test the hypothesis generated on the basis of the time, place and person description C.I.: Confidence interval
3. Monitoring the situation • Trends in cases and deaths • Implementation of containment measures • Stocks of vaccines and drugs • Logistics • Communication • Vehicles • Community involvement • Media response
4. Declaring the outbreak over • Role of the district surveillance officer / Medical health officer • Criteria • No new case during two incubation periods since onset of last case • Implies careful case search to make sure no case are missed
5. Review of the final report • Sent by medical officer of the primary health centre to the district surveillance officer / medical and health officer within 10 days of the outbreak being declared over • Review by the technical committee • Identification of system failures • Longer term recommendations
Managerial aspects of outbreak response • Logistics • Human resources • Medicines • Equipment and supplies • Vehicle and mobility • Communication channels • Information, education and communication • Media • Daily update
Control measures for an outbreak • General measures • Till source and route of transmission identified • Specific measures, based upon the results of the investigation • Agent • Removing the source • Environment • Interrupting transmission • Host • Protection (e.g., immunization) • Case management
Specific outbreak control measures • Waterborne outbreaks • Access to safe drinking water • Sanitary disposal of human waste • Frequent hand washing with soap • Adopting safe practices in food handling • Vector borne outbreaks • Vector control • Personal protective measures • Vaccine preventable outbreaks • Supplies vaccines, syringes and injection equipment • Human resources to administer vaccine • Ring immunization when applicable
Reports • Preliminary report by the nodal medical officer (First information report) • Daily situation update • Interim report by the rapid response team • Final report
Points to remember • Outbreaks cause suffering, bad publicity and cost resources • Constant vigil is needed • Prompt timely action limits damage • Emphasis is on saving lives • Don’t diagnose every case once the etiology is clear • Management of linked cases does not require confirmation • The development of an outbreak is followed on a daily basis • Effective communication prevents rumours • Use one single designated spoke person • Learn lessons after the outbreak is over