Download
1 / 53
530 likes | 892 Views
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE. Core Interventions in the Treatment and Management of Schizophrenia in Primary and Secondary Care Guidance on the use of the newer (atypical) antipsychotic drugs for the treatment of schizophrenia John Rawlinson Andy Carberry. Context. CPA 1990,

E N D
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE • Core Interventions in the Treatment and Management of Schizophrenia in Primary and Secondary Care • Guidance on the use of the newer (atypical) antipsychotic drugs for the treatment of schizophrenia John Rawlinson Andy Carberry
Context • CPA 1990, • Health of the Nation (DoH 1992) • ‘Serious and Enduring Mental Illness’ and suicide risk • Clinical Standards Advisory Group - Schizophrenia (CSAG 1995) • Family, PSI, Pharmacology, EI, AO, etc, • Evidence Based Practice (EBM/EBP)
Context (cont.) • Effective Health Care Bulletins, Cochrane Reviews etc. (1999-2002) • National Service Framework for Mental Health (DoH 1999) • ‘Recent advances in understanding mental illness and psychotic experiences’ (BPS 2000) • Mental Health Policy Implementation Guide and other PIGs (DoH 2001on)
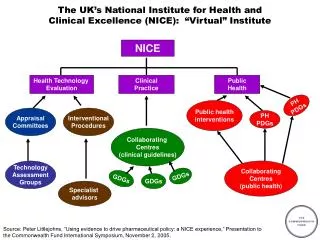
Context (cont.) • Guidance on the use of newer (atypical) antipsychotic drugs for the treatment of schizophrenia (NICE 2002) • Core Interventions in the treatment and management of schizophrenia in primary and secondary care (NICE 2002) <http://www.nice.org.uk> NHS Responseline: 08701 555 455 <doh@prologistics.co.uk>
Policy Implementation Guidelines (PIGs) Can we make them a reality ?
Outcomes of schizophrenia • 22-25%: Have a single diagnosed episode with no resulting clinical or social impairment • 35%: Have occasional recurrences with no or minimal impairment between episodes • 8%: Experience some social impairment after the first acute episode persisting unaffected by further breakdowns
Outcomes of schizophrenia (cont.) • 35%: Are increasingly damaged by each subsequent acute crisis so that social functioning worsens progressively • 50% Of those treated in standard services relapse requiring readmission in the first 2 years (1% lifetime risk in general population across all cultures) Frangou and Murray 1996, Mason et al 1996 in NICE2002
Other outcomes of schizophrenia • Negative social reactions to symptoms and behaviour, with consequences such as stigma, discrimination, high unemployment, failed or impoverished relationships etc.. • 10 years shorter lifespan than the general population
Other outcomes of schizophrenia (cont.) • 10% of those diagnosed with schizophrenia commit suicide • Significantly higher risk of Accidents and Cardio-vascular disease Frangou and Murray 1996
Principles of NICE care • Optimism • Getting help early • Comprehensive Assessment - medical, psychological, occupational, economic, physical and cultural • Partnership with users and carers • Consent and engagement • Good information and mutual support
Principles of NICE care (cont.) • Language and culture • Advance directives
Care across three phases • Initiation of treatment at the first episode • Acute phase • Promoting recovery
Initiation of treatment (First episode) • Early Referral All people with suspected or newly diagnosed schizophrenia presumed diagnosis of schizophrenia - assessment by a Consultant Psychiatrist.
Initiation of treatment (First episode) • Early Intervention Early Intervention Services Where needs of the user exceeds capacity, referral to crisis resolution/ home treatment/ acute day services/ inpatient services
Initiation of treatment (First episode) • Pharmacological Interventions Oral atypical antipsychotic drugs choice of first time treatments at the lower end of the standard dose range.
Initiation of treatment (First episode) • Second Opinion Support a decision by a service users to seek a second opinion
Treatment of the acute episode • Service level intervention • Pharmacological intervention • Broad range of social, group and physical activities essential elements • Mental Health Act and or inpatient treatment may prove necessary
Service level interventions • crisis resolution • home treatment teams • early intervention and YP services • assertive outreach • community mental health teams • acute day hospitals • in patient care
Core interventions in the management of schizophrenia Early Post acute period • User focus • Assessment • Psychological treatments including CBT and family work • Medication advice Promoting Recovery - Primary and Secondary services Preventing Relapse - ongoing psychological and pharmacological intervention
Early post-acute period care • Help to users better understand the period of illness, and be given the opportunity to write their account in their notes. • Carers may need help in understanding the experience. • Assessment for further help to minimise disability, reduce risk and improve quality of life.
Early post-acute period care • Psychological and family help, contingency planning and identify local resources/services • Advice about drug treatments to maintain recovery
Promoting recovery • Primary care • Secondary care • Service Interventions • Psychological interventions • Pharmacological interventions • Employment
Cognitive Behaviour Therapy • Cognitive behavioural therapy (CBT) should be available as a treatment option for people with schizophrenia - A • In particular, cognitive behavioural therapy should be offered to people with schizophrenia who are experiencing persisting psychotic symptoms - A
Family Interventions • Family interventions should be available to the families of people with schizophrenia who are living with or who are in close contact with the service user – A
Pharmacological intervention - all phases • Antipsychotic drugs are necessary. • Service users should make an informed choice of antipsychotic • Single drug, using doses within the BNF dose range • Clinical response and side effects monitored routinely and regularly.
Pharmacological intervention - all phases • Oral atypical drugs should be considered as the treatment option of choice • Dosage of conventional antipsychotic in the range of 300-1000mg Chlorpromazine equivalents/day for a min. 6 weeks. Reasons for doses outside this range should be justified and documented. The minimum effective dose should be used. • If side effects are troublesome or symptom control inadequate, atypical should be offered.
Pharmacological intervention - all phases • Massive loading doses “rapid neuroleptization” should not be used. • Rapid tranquillisation may be required in the acute phase (lorazepam, haloperidol or olanzapine) (see section 1.5)
Pharmacological intervention recovery phase Relapse prevention – oral antipsychotic • Antipsychotic drugs are indispensable option for most people in the recovery phase • Choice of antipsychotic made jointly by individual and clinician • Antipsychotic therapy part of a comprehensive package of care that addresses clinical emotional and social needs.
Pharmacological intervention recovery phase Relapse Prevention – depot antipsychotic • A risk assessment should be performed • Initiation of depot antipsychotic injection should take into account the preferences and attitudes of the service user
Pharmacological intervention recovery phase Treatment – Resistant Schizophrenia • Antipsychotic drugs adequately tried - dosage, duration, adherence. • Atypical antipsychotic in advance of diagnosis of treatment resistant schizophrenia. • Treatment resistant schizophrenia - Clozapine
NICE - The Evidence • Evidence to support core interventions in the treatment and management of schizophrenia in primary and secondary care
Type of evidence • 1a - Evidence obtained from a single large randomised trial or meta-analysis of at least 3 RCT’s. • 1b - Evidence obtained from a small randomised controlled trial or a meta-analysis of less than 3 RCT’s.
Pharmacological Interventions • 172 RCT’s reviewed with evidence from 29 ‘head to head’ trials of typical agents. • In addition 53 other studies were considered which were either case control, had more than 2 years of follow up, or included more than 2000 participants. • The overwhelming majority of RCT’s were 4 to 8 weeks long with 31 being over 6 months duration.
Considerations • Limited by lack of long term follow up, high attrition rates and the inadequacy of the collection and reporting of adverse effects. • Haloperidol which may be associated with a higher rate of EPS than other typicals was used as the comparitor in many of the trials.
The generalisability of individual study results was limited by the exclusion of elderly people as well as individuals with TRS, predominantly negative symptoms, learning disabilities, co-morbid depression and substance abuse disorders.
Evidence • Atypical antipsychotics are at least efficacious as the typical agents in terms of overall response rates. • Variation in their relative effects on positive and negative symptoms and relapse rates. • Inadequate data to enable separate evaluation of the overall impact of individual atypicals on schizophrenia.
Evidence • All atypicals are associated with a reduced incidence of EPS compared to typicals in the short to medium term (up to 26 weeks). In the long term (26 weeks or longer) there are limited data to support a reduced incidence of EPS with some of the atypicals. • Little evidence of comparative rates of tardive dyskinesia between the atypicals or between the typical and atypicals.
Evidence • The side effect profiles of individual atypicals may differ but definitive statements relating to differences between them are difficult to make because of variations in the evidence base for individual drugs and in the length of treatment follow up.
Clozapine • Evidence suggests that in individuals who have not responded to previous antipsychotic therapy then clozapine is associated with fewer relapses and greater clinical improvement than typical agents.
Recommended Drugs • Amisulpride • Olanzapine • Quetiapine • Risperidone • Zotepine
Cognitive Behavioural Therapy • Total of 13 RCT’s included in the review, providing data on 1297 participants. All in these trials were also receiving antipsychotic drugs, and most often CBT was targeted at individuals with long standing or treatment resistant psychosis. Control groups received ‘standard care’, recreational activities, befriending or supportive counselling.
Effect of CBT upon suicide & relapse rates Insufficient evidence - • When compared to ‘standard care’ during treatment -1b • When compared to ‘standard care’ at 12 months post-treatment follow up - 1b • When compared to other psychological treatments at 1-2 years post-treatment follow up - 1a.
Effect of CBT upon symptoms • Limited evidence that CBT reduces symptoms when compared to ‘standard care’ at end of treatment - 1b. • Strong evidence that CBT improves mental state when compared to ‘standard care’ at end of treatment - 1a. • Limited evidence that CBT reduces symptoms when compared to other psychological interventions at the end of treatment - 1b.
Other effects of CBT • Adherence to drug treatment when compared to ‘non specific counselling’- 1b. • Improvements in insight, compared to other treatments, at 12 months and 5 year follow up - 1b. • Improvements in social functioning, when compared to ‘non standard care’ - 1b.
Clinical summary -CBT Overall there is good evidence that CBT reduces symptoms for people with schizophrenia at up to 1 year follow up when compared to ‘standard care’ and other treatments. The evidence is stronger when CBT is used for the treatment of persisting psychotic symptoms rather than for acute symptoms.
Family Interventions Family sessions with a specific supportive or treatment function based on systemic, cognitive behavioural or psychoanalytic principles which must contain at least 1 of the following - • Psycho-educational intervention. • Problem solving/crisis management work. • Interventions with the service user
Evidence • 18 RCT’s with data for 1458 study participants and their families. Comparator interventions included ‘standard care’ (11 studies), or ‘non standard care’ (standard care plus general family support - 5 studies)
Results • There is strong evidence that family interventions, when compared to all other interventions, decrease the likelihood of: • Relapse during treatment - 1a. • Relapse 4 to 15 months post-treatment follow up - 1a. • Hospital admission 13 to 24 months into treatment - 1a.
Results • There is limited evidence that family interventions, when compared to all other treatments, reduce the likelihood of: • Relapse in people with persisting symptoms, after 12 months of treatment - 1b. • Relapse in people with persisting symptoms up to 6 months post-treatment - 1b.