Download

1 / 49
520 likes | 718 Views
Acne. By Sapna Prabhakaran, MD. Objectives. Types Diagnosis Treatments. Types.

E N D
Acne By Sapna Prabhakaran, MD
Objectives • Types • Diagnosis • Treatments
Types • Neonatal – may occur at birth, usu. occurs at 2-3 weeks of age, cause not known but some believe it’s from maternal androgens and others propose it’s an inflammatory response to resident yeast, s/s: inflammatory erythematous papules and macules, rarely comedones, primarily in the cheeks, rare on the trunk tx: spontaneous resolves • Infantile - usually around 2-3 months of age, may represent persistance of neonatal acne or a true acne variant, usually resolves by 6-12 months of age similar to neonatal acne but comedones maybe present tx: topical 2.5% benzoyl peroxide or topical 2% erythromycin solution or gel or topical retinoids such as adaplene • Acne vulgaris
Acne Vulgaris • Epidemiology of acne vulgaris • Most common skin disease that is treated by physicians • Affects about 45 million individuals in the US, including at least 85% of all teenagers and young adults • Has the potential for significant negative impact on quality of life
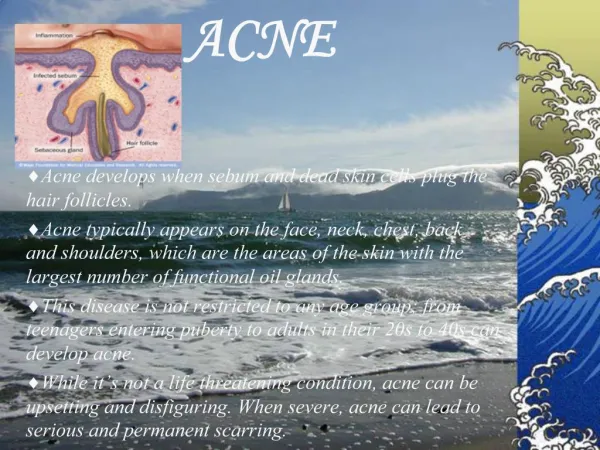
Pathophysiology • Result of a complex interaction between hormonal changes and their effects on the pilosebaceous unit - specialized structures consisting of a hair follicle and sebaceous glands that are concentrated on the face, chest and back • Onset at puberty because of increased androgen production • Disordered function of the pilosebaceous unit with abnormal follicular keratinization (tendency toward increased follicular plugging)
Pathophysiology • Increased density of Propionibacterium acnes, a normal resident of the skin • Increased sebum production, under the influence of adrenal and gonadal androgens • Breakdown of sebum by P acnes results in production of proinflammatory mediators, which leads to the development of the characteristic inflammatory lesions
Pathophysiology Factors • Factors that may exacerbate acne • Trauma – scrubbing the skin too vigorously or picking of lesions • Comedogenic cosmetics or other skin care products • Tight fitting sports equipment • Medications: corticosteroids and anabolic steroids, antiepileptic drugs, lithium and certain contraceptives • Hormonal dysregulation as in conditions like PCOS or Cushing syndrome
Signs and Symptoms • Early on, acne lesions often appear on the forehead and middle third of face (T-zone) and are obstructive; inflammatory lesions tend to develop later and lesions may occur on all areas of the face, neck, chest and back • Comedones and inflammatory lesions • Open comedones – blackheads: dilated follicles • Closed comedones – (whiteheads): white or skin colored papules without surrounding erythema
Signs and Symptoms Inflammatory lesions typically appear later in the course of acne vulgaris and vary from 1-2mm micropapules to nodules larger than 5mm • Large (5-15mm) inflammatory nodules and cysts occur in most severe cases and such nodulcystic presentations are most likely lead to permanent scarring • Mild, moderate and severe inflammatory acne can be associated with disfiguring post-inflammatory discoloration, which can be red, violaceous or grey-brown hyperpigmentation • Pigmentary lesions may persist for many months
Treatment • 4-6 weeks or longer maybe required to observe a benefit from treatment • Optimize skin care - use a facial cleanser that has salicylic acid or benzoyl peroxide, if using prescription products, then want to use a mild cleanser • Classify acne into mild moderate and severe to be able to pick the appropriate treatment regimen
Treatment • Treatment strategies are based on severity of disease • Mild acne – (face: one fourth of the face is involved, few to several papules or pustules, but no nodules or scarring) • Topical therapy are usually adequate as an initial intervention and include a choice of topical retinoids, topical benzoyl peroxide, and topical benzoyl/antibiotic combinations • Retinoid pearls – • apply to a dry face • apply no more than a pea size amount for the entire face • If the entire face needs to be covered - touch pea size aliquot to each side of forehead, each cheek and chin and rub it in • Apply to all areas and not as spot therapy • Use a noncomedogenic moisturizer sparingly to counteract the dryness assoc with retinoid therapy
Treatment • Moderate acne ( face: about one half of the face to be involved; there are several to many papules or pustules and a few to several nodules; a few scars maybe present) • Benzoyl peroxide/topical antibiotics combination products, along with topical retinoids, are an effective treatment strategy – one is applied in the morning and one is applied in the evening • Another option is a topical antibiotic and a topical retinoid • If inflammatory lesions are present , use of oral antibiotics should be added but still need to add benzoyl peroxide because has shown that benzoyl peroxide decreases risk of developing antibiotic resistance • Female patients who have significant inflammatory acne, particularly those who have premenstrual or menstrual flares, may benefit from hormonal intervention such as oral contraceptive pills
Treatment • Severe acne (face: three fourths or more of the face is involved; there are many papules and pustules, and many nodules; scarring is present) • Nodulocystic acne or the presence of scarring warrant prompt consideration for isotretinoin therapy( with referral to a dermatologist) • High dose oral antibiotics in combination with topical therapy is an option while considering isoretinoin.
BENZOYL PEROXIDE • Antibacterial and mild comedolytic • Ubiquitous treatment for inflammatory and non-inflammatory acne • Formulations: 2.5, 5, and 10% gels, lotions and creams • Risks: irritation, contact dermatitis, and bleaching of clothes • Pearl: start low, brief application during initial days of treatment: 15-30 minutes/day
RETINOIDS • Normalizes follicular keratinization • Resolves matures comedones • Prevents new lesions • Enhances penetration of other drugs • Basically reverse the ‘stickiness” of the skin cells, allowing them to slough normally
TRETINOIN (RETIN-A) • Comedolytic • Best topical treatment for comedones • Risks: irritation, photosusceptability, hyperpigmentation • Formulations: 0.01, 0.025, 0.05, 1% gel, cream • Pearl: bedtime use, brief application during initial phase of treatment
TOPICAL ANTIBIOTIC • Clindamycin • Antibacterial • Risks: irritation, rare report of pseudomembranous colitis • Formulation: gel,lotion and newer foam (Cleocin)
SYSTEMIC ANTIBIOTICS • Tretracycline • Antibacterial • 500mg BID • Inhibits chemotaxis of neutrophils (anti-inflammatory effect • Photosensitivity, GI irritation, vaginal candidiasis, teratogenic; possible reduced effect of OCPs • Take ½ hr before, or 2hrs after meal
TRIAZ • Benzoyl peroxide, glycolic acid, zinc • Anti-microbial, anti-comedonal • 3, 6 and 9% • Less irritation • Also successful in pseudofolliculitis barbae
BENZACLIN • BP 5%-clindamycin combination • Maybe used in lieu of oral antibiotics in mild papular, pustular acne • Benzamycin (erythromycin/BP combination) • Duac (clinda/BP)
ZIANA • Clindamycin/tretinion combo • Antibacterial/comedolytic • Risks: irritation, GI effects of clinda • Expensive
ADAPELENE (DIFFERIN) • Synthetic napthalene retinoid derivitive • Anti-comedones, some anti-inflammatory • Risks: irritation 10-40%; photosusceptible, hyperpigmentation
RETIN A-MICRO • Different formulation of Retin-A • Anti-comedonal with less irritation
TAZAROTENE (TAZORAC) • Retinoid derivitive • Anti-comedonal, anti-inflammatory, anti-proliferative • Also used in psoriasis • Irritation 10-30%; • Start brief contact, 2-5 minutes BID
AZELAIC ACID (AZELEX) • Dicarboxylic acid • Antimicrobial, anti-keratinization • Decrease hyperpigmentation • 20% Cream BID dosing • Useful in pts that prone to hyperpigmenation
MINOCIN (MINOCYCLINE) • Special acne indication • 50mg BID dosing • Risks: gray-blue discoloration of skin; hepatitis; lupus like illness
DOXYCYCLINE • Low dose formulation • Periostat 20mg BID • Likely anti-inflammatory effect • More expensive than regular hight dose doxy
BACTRIM • DS BID used 2-3 months • Moderate severe cases • Consider prior to using accutane
ZITHROMAX • Pavone-Italy: • 500mg qd x 3 days, then 7 days off, for 3 cycles • Schachner, Miami: • Z-pak x 5days, then 1 month off • Elewski, Miami: • Z-pak during menstrual flares
ISOTRETINOIN (ACCUTANE) • Most effective agent for severe inflammatory acne or nodularcystic acne • Only drug that affects all pathogenic factors • Anti-comedonal, anti-bacterial, anti-inflammatory, decrease sebum production; • Teratogenic, anemia, thrombocytopenia, hepatitis, ocular/vaginal dryness, arthralgia, pseudotumor cerebri, depression • Can have granulomatous reaction initially (can use prednisone) • Dermatology/national registry
OCP • Ortho-tri-cyclen, Yaz, Yasmin • Risks: nausea, vaginal bleeding • Consider using in mod-severe inflammatory acne • Trial prior to Accutane
Prognosis • Acne vulgaris is often self limited and resolves by late teenage or early adult years • Treatment is warranted during periods of disease activity to alleviate disfigurement, enhance well being and prevent scarring. • Referral to dermatology is recommended after failure to respond topical and/or oral therapies after 2-3 months of appropriate use • Severe acne with presence of nodules, cysts and/or scarring
Conclusion • Thanks for your time !!!