Download
1 / 33
630 likes | 1.18k Views
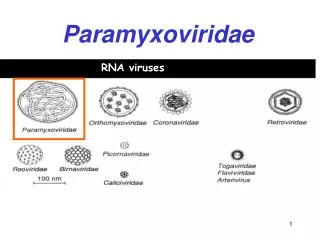
Paramyxoviridae. 150-200 nm . Large virions consists of a negative strand RNA genome in a helical nucleocapsid surrounded by an envelope containing a viral attachment protein and a fusion glycoprotein (F). Mediates Fusion 0f infected cellss yncytia. HN. H. Morbillivirus.

E N D
150-200 nm Large virions consists of a negative strand RNA genome in a helical nucleocapsid surrounded by an envelope containing a viral attachment protein and a fusion glycoprotein (F). Mediates Fusion 0f infected cellss yncytia
HN H Morbillivirus Paramyxovirus RSV Measles paramyxoviridae Pneumovirus • Parainfluenza (1-4) • Mumps 1&2chld&inf 3 >2 y severe 4-Mild disease
General features on Paramyxoviridae family • Viruses replicate in the cytoplasm. • Viruses induce cell-cell fusion via F protein, causing multinucleated giant cells (Syncytia). • Paramyxoviridae are transmitted in respiratory droplets and initiate infection in the respiratory tract. • Cell-mediated immunity, causes many of the symptoms but is essential for control of the infection. • Measles and mumps produce a viremia and thereafter a generalized infection; RSV and parainfluenza viruses produce only respiratory infection.
Parainfluenza • Parainfluenza viruses cause mild or severe upper and lower respiratory tract infections, particularly in children. • 1&2 Croup, boys>girls • 1/3 of all RTI & 1/5 of RTI in pre-school children and infant • Type 3 LRT (bronchitis & pn) • Transmission is by droplets or direct contact. The virus disseminates locally in the ciliated epithelial cells of the respiratory mucosa.
Clinical feature • The syndrome develop rapidly with bursts of harsh • Barking cough with noisy breathing • Many cases are mild • Restlessness & tachycardia increase as respiratory obstruction develops • If bronchi loaded with mucus- auscultation of the chest • Syanosis is late • Most cases resolve within a week, croup cough may return if respiratory infection followed
Management Warm & steamy atmosphere Dexamethasone 4-8 mg twice/day improve airway function
Mumps • Old name mean (to mope (depressed persons • Acute viral infection that primary infect parotid gland • Immunity is life-long after a case of mumps • 1/3 sub clinical
Local replication Systemic infection Viremia Inoculation EC of URT Testes Ovaries Peripheral nerves Eye Inner ear CNS Parotid gland pancreas Virus multiplies in ductal epithelial cells. local inflammation causes Marked swelling Time course of Mumps infection
Mumps is infectious for 2 -7 days before the symptoms and for approximately 9 - 10 days after the appearance of the symptoms.
Clinical aspects • Often asymptomatic • Malaise and fever followed (24h) by • redness & swelling of parotid gland duct (Parotitis) • Swelling of other glands • Complication • Menengoencephalitis may occur • Swelling of orchitis cause sterility (20%) 2-5 days after parotitis and subset after 3-6 days • Inflammation of the ovary (oophoritis) • 50% may involve CNS
Measles • Serious and highly contagious • Usually found in non-immunized or partially-immunized (single vaccine, no booster) • Most born before 1957 have had measles • Measles virus is spread easily • Through air by coughs or sneezes • By direct contact with nose or throat secretions • Symptoms • Rash that starts on the face and neck, then spreads • High fever • Runny nose • Red, watery eyes • Cough
Measles • Symptoms start about 10 days after exposure • Average 10 days from exposure to onset of fever • Average 14 days from exposure to onset of rash • Other symptoms and complications • Ear infection • Pneumonia • CNS/ brain infection (as SSPE, subacute sclerosing panencephalitis) • Complications may be lethal • More serious in infants and adults, less in children and teens • Vaccine • Measles (Paramyxoviridae), mumps (Paramyxoviridae), rubella (Togaviridae, + sense) (MMR) vaccine is a live vaccine • Has been very effective in limiting spread • Links of vaccine to autism have been proposed but not shown Management Antibiotics should be used to combat side-effects such as ear infetions pneumonia. Giving vitamin A at the time of diagnosis can help to prevent blindess
اheight of fever Running E&N,cough & fever, replicate WBC Face-trunk 40 Satisfactory immu respo & recov
Lymphatic spread Wide dissemination Virus- infected endothelial cells+ immune T cell Measles pathogenesis
Respiratory Syncytial Virus Family Paramyxoviridae Genus Pneumovirus Subgroups A and B
Localised infection of RT Pneumonia from cytopathologic spread Not causing Viremia Pathogenesis Bronchiolitis from host immune response Narrow airways of infants obstructed by virus-induced pathologic effect Maternal antibody does not protect infant from infection
Entry through mucosa of nose and eye Cell to cell spread within respiratory tract Pathogenesis Attachment via G protein to respiratory epithelium Fusion with cell membrane - F protein Syncytium formation (tissue culture) with multinucleated giant cells
Clinical Features Upper Respiratory Infection • Fever • Rhinitis • Pharyngitis Lower Respiratory Infection- Bronchiolitis, Pneumonia • Cough • Poor feeding, lethargy • Hypoxemia • Respiratory Distress (tachypnea, retractions) • Apnea
RSV- Severe Disease • Preterm Infants • Chronic Lung Disease, Bronchopulmonary dysplasia (BPD) • Cyanotic congenital heart disease • Congestive heart failure • Immunocompromised patients • Neurologic or metabolic diseaes
Diagnosis- RSV in Hep-2 cell culture(immunofluoresent stain)
Clinical Course in Adults • Viral shedding usually lasts 3-6 days, with a range of 1 to 12 days • In patients with underlying malignancy and suppressive chemotherapy, prolonged viral shedding is seen. • the mortality is estimated at 51% in patients with bone marrow transplants
Diagnosis • Nasal Wash, throat swab, tracheal aspirate specimens • Hep-2 cells show typical colony formation, confirmed with immunofluorescent staining • Sensitivity and Specificity of Rapid antigen assays >90%
Treatment • Supportive Care with bronchodilators and oxygen supplementation, ventilatory support • Half of patients with leukemia as underlying diagnosis require ventilatory support • Steroids—no change in clinical course of RSV, but may be used in setting of bronchospasm
Antiviral Therapy • Ribavirin– Largest study included 13 treated patients (70% mortality) and 5 untreated patients (100%) during an outbreak in a bone marrow transplant center.
RSV Spectrum of Disease • Mild respiratory illness in adults • Common Cold • Severe Disease in infants , premature and immunocompromised • Bronchiolitis • Pneumonia Seasonal variation common in spring
Laboratory Diagnosis 1. Viral Detection Isolation of a paramyxovirus from a patient is strong evidence for a cause of a respiratoyr infection. (All the Paramyxoviruses are to be found in the respiratory tract secretions - and this is the best material to send to the laboratory). The paramyxoviruses are unstable and do not survive well outside cells. a) Direct Examination -Viral antigens detected by ELISA tests. -viral infected cells in the secretions can be detected b immunofluorescence
2. Serological Diagnosis Antibody determinations in acute and convalescent blood specimens by complement fixation, Elisa or haemagglutination inhibition may sometimes be helpful in arriving at a specific diagnosis.Respiratory syncytial virus and measles virus infections are fairly clearcut.Mumps and Para influenza viruses seem to share a group common antigen (cross reactivity), and serological interpretation may be difficult.