Download
1 / 20
290 likes | 845 Views
Development of the Foregut 2. Dr Rania Gabr. Objectives. Describe the development of the Duodenum. Describe the development of the Liver and gall bladder. Describe the development of the Pancreas. Identify the congenital anomalies of the duodenum, liver and pancreas. Duodenum.

E N D
Development of the Foregut 2 Dr Rania Gabr
Objectives • Describe the development of the Duodenum. • Describe the development of the Liver and gall bladder. • Describe the development of the Pancreas. • Identify the congenital anomalies of the duodenum, liver and pancreas.
Duodenum • Formed from the terminal part of the foregut and cranial part of the midgut. • Origin of the liver bud marks the junction of 2 parts of the gut. • Initially, the duodenum is a straight tube, but due to the rotation of stomach, duodenum assumes a C-shaped structure and lies to the right. • The head of the pancreas grows into the concavity of the duodenum.
DEVELOPMENT OF THE DUODENUM • Early in the 4th week, the duodenum develops from the endoderm of primordial gut of the: • Caudal part of foregut. • Cranial part of midgut & from :Splanchnic mesoderm. • The junction of the 2 parts of the gut lies just below or distal to the origin of bile duct (C &D). 4th week 5th week
6thweek 5th week 6th week
DEVELOPMENT OF THE DUODENUM • The duodenal loopis formed and projected ventrally, forming a C-shaped loop (C). • The duodenal loopis rotated with the stomach to the right and comes to lie on the posterior abdominal wall retroperitoneally with the developing pancreas. 4th week 5th week 6th week 5th week
Development of the duodenum • During 5th & 6th weeks, the lumen of the duodenum is temporarily obliterated because of proliferation of its epithelial cells. • Normally degeneration of epithelial cells occurs, so the duodenum normally becomesrecanalizedby the end of the embryonic period.
Congenital anomalies Duodenal stenosis; results from incomplete recanalization of the duodenum. Duodenal atresia; results from failure of recanalizationleadingto complete occlusion of the duodenal lumen, (autosomal recessive inheritance ).
Liver and gall bladder • The liver bud (endodermal) grows from the terminal part of the foregut during the middle of the third week. • This bud with proliferating cells grows into the septum transversum (mesodermal). • The connection between the cellular proliferation and foregut narrows and becomes the bile duct.
Liver and gall bladder • A cystic bud grows from the bile duct to form the gall bladder and cystic duct. • The hepatocytes develop from the endoderm. • The blood cells, Kupffer cells and connective tissue and its cells develop from the mesoderm of the septum transversum.
Liver and gall bladder abnormalities • Accessory hepatic ducts: common variation. • Duplication of gall bladder:common variation.
Extrahepatic biliary atresia: 1/15,000 live births. Due to failure in re-canalization of duct during development. • Intrahepatic biliary atresia: biliary duct inside liver is not canalized
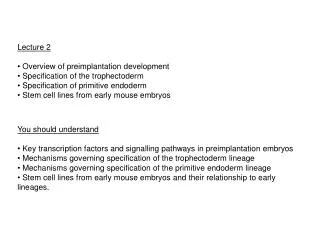
DEVELOPMENT OF PANCREAS Ventral mesentry • The pancreas develops from 2 buds arising from the endoderm of thecaudal part of foregut : • A ventral pancreatic bud :which develops from the proximal end of hepatic diverticulum (forms the liver & gall bladder). • A dorsal pancreatic bud :which develops from dorsal wall of duodenum slightly cranial to the ventral bud. • Most of pancreas is derived from the dorsal pancreatic bud. Dorsal mesentry
A. A 9-mm embryo (approximately 36 days). B.A slightly older embryo.
DEVELOPMENT OF PANCREAS • The ventral bud rotates to the left and lies below the dorsal bud. • Both buds fuse and form the pancreas. • The ventral bud forms : • Uncinate process. • Inferior part of head of pancreas. • The dorsal pancreatic bud forms : • Upper part of of head. • Neck, Body &Tail of pancreas.
DEVELOPMENT OF PANCREAS • The main pancreatic duct is formed from : • The duct of the ventral bud. • The distal part of duct of dorsal bud. • The accessory pancreatic duct is derived from : • Proximal part of duct of dorsal bud. • The parenchyma of pancreasis derived from the endoderm of pancreatic buds. • Pancreatic isletsdevelops from parenchymatous pancreatic tissue. endoderm • The connective tissue of the gland develops from the splanchnic mesoderm. • Insulin secretionbegins at 5th month of pregnancy.
Congenital anomalies Accessory pancreatic tissue; located in the wall of the stomach or duodenum or Mickel`s diverticulum. Anular pancreas; a thin flat band of pancreatic tissue surrounding the second part of the duodenum, causing duodenal obstruction.