Download
1 / 35
350 likes | 355 Views
This article discusses the laboratory examination methods for the diagnosis of autoimmune diseases, such as rheumatoid arthritis and systemic lupus erythematosus. It also explores the role of genetic factors, environmental exposure, and breaking tolerance in the development of autoimmunity.

E N D
Laboratory examination in Immune disorders Umi S. Intansari Bag. Patologi klinik FK UGM/ RSUP Dr. Sardjito Yogyakarta
c c c c c c c c Mackay IR, 2000, BMJ 321: 93-96
A critical function of the immune system is to discriminate self from non-self
Requirement for autoimmunity Infection and environmental exposure Genetic factors Breaking tolerance Autoimmunity
Faktor genetik DM tipe 1 HLA DR3/4 increase susceptibility of disease in type 1 DM Autoimmunity is more common in female Shared HLA in sibling increase susceptibility of disease in type 1 DM
Prevalence of autoimmune diseases • Rheumatoid arthritis: 1% of general population, but female excess • SLE: 0.12% of general population, but female excess • Myasthenia gravis: 0.0% of general population, but female excess • Multiple sclerosis: 0.1% of general population but female excess • Primary Sjogren Syndrome: 0.6-3% of adult women • Thyroid disease: >3% of adult women • Type 1 diabetes: 0.1% of children Mackay IR, 2000, BMJ 321: 93-96
Deteksi autoantibodi • Ada bermacam-macam antibodi terhadap antigen intraseluler dan nuklear • Deteksi dapat dilakukan secara kualitatif, kuantitatif dan dilanjutkan identifikasi spesifikasi imunologisnya • Secara umum dikarakterisasi oleh; • Ada tidaknya antibodi spesifik • Perbedaan level kuantitatif/titer dari autoantibodi
Revised ARA Criteria for the Classification of Rheumatoid Arthritis (RA) For classification purposes, a patient is said to have RA if he or she has satisfied at least 4 of the following 7 criteria. Criteria 1 through 4 must have been present for at least 6 weeks. Patients with 2 clinical diagnoses are not excluded. Designation as classic, definite, or probable RA is not to be made. Morning stiffness: Morning stiffness in and around the joints, lasting at least 1 hour before maximal improvement. Arthritis of 3 or more joint areas: At least 3 joint areas simultaneously have had soft tissue swelling or fluid (not bony overgrowth alone) observed by a physician; the 14 possible joint areas are right or left proximal interphalangeal (PIP) joints, metacarpophalangeal (MCP) joints, wrist, elbow, knee, ankle, and metatarsophalangeal (MPT) joints. Arthritis of hand joints: At least I area swollen (as defined above) in a wrist, MCP or PIP joint. Symmetric arthritis: Simultaneous involvement of the same joint areas (see 2 above) on both sides of the body (bilateral involvement of PIPs, MCPs, or MTPs is acceptable without absolute symmetry). Rheumatoid nodules: Subcutaneous nodules, over bony prominences, or extensor surfaces, or in juxta-articular regions, observed by a physician. Serum rheumatoid factor: Demonstration of abnormal amounts of serum rheumatoid factor by any method for which the result has been positive in <5% of normal control subjects. Radiographic changes: Radiographic changes typical of RA on posteroanterior hand and wrist radiographs, which must include erosions or unequivocal bony decalcification localized to or most marked adjacent to the involved joints (osteoarthritis changes alone do not qualify).
Systemic Lupus Erythematosus (SLE) Autoantibody-mediated inflamation can lead to release of autoantigens from damaged tissue and promotes further activation o f autoreactive B cells Chronic stage
Classification Criteria for the Diagnosis of Systemic Lupus Erythematosus (SLE) Malar rash: Fixed erythema, flat or raised, over the malar eminences Discoid rash: Erythematous circular raised patches with adherent keratotic scaling and follicular plugging; atrophic scarring may occur Photosensitivity: Exposure to ultraviolet light causes rash Oral ulcers: Includes oral and nasopharyngeal ulcers, observed by physician Arthritis: Nonerosive arthritis of two or more peripheral joints, with tenderness, swelling, or effusion Serositis: Pleuritis or pericarditis documented by ECG or rub or evidence of effusion Renal disorder: Proteinuria >0.5 g/d or 3+, or cellular casts Neurologic disorder: Seizures or psychosis without other causes Hematologic disorder: Hemolytic anemia or leukopenia (<4000/L) or lymphopenia (<1500/L) or thrombocytopenia (<100,000/L) in the absence of offending drugs Immunologic disorder: Anti-dsDNA, anti-Sm, and/or anti-phospholipid Antinuclear antibodies: An abnormal titer of ANA by immunofluorescence or an equivalent assay at any point in time in the absence of drugs known to induce ANAs Any combination of 4 or more of 11 criteria, well-documented at any time during a patient's history, makes it likely that the patient has SLE (specificity and sensitivity are 95% and 75%, respectively). Note: ECG, electrocardiography; dsDNA, double-stranded DNA; ANA, antinuclear antibodies.
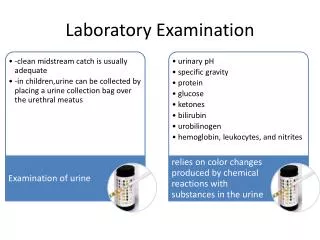
Lupus eritematosus sistemik (SLE) Pem urin kuantitatif Urin rutin The American College of Rheumatology ( ACR ) established 11 criteria in 1982, which were revised in 1997
Darah lengkap, urin rutin, Comb’s test, Morfologi Darah Tepi Retikulosit, LDH, bilirubin Sel LE, Anti Sm, anti Ds DNA, VDRL, TPHA ANA tes The American College of Rheumatology ( ACR ) established 11 criteria in 1982, which were revised in 1997
Immunofluorescence microscope Indirect immunofluorescence of ANA (homogenous pattern Courtesy: Stanford Clinical chemistry web Fluorescence imaging of renal biopsy of lupus nephritis patient (SLE Courtesy: NUS home page
Coombs tests and the detection of Rh incompatibility Use anti-immunogobulin antibodies (Coombs reagent) to detect antibodies that cause disease Direct : directly detect Ab bound to the surface of fetal red blood cells Indirect: detect nonagglutinating anti-Rh Ab in maternal serum 19
Figure A-13 21
Alergi dan hipersensitivitasdefinisi Hipersensitivitas adalah reaksi imun terhadap antigen lingkungan yang sebenarnya tidak berbahaya yang mengakibatkan kerusakan jaringan dan/ atau penyakit Alergi adalah salah satu dari reaksi hipersensitivitas: reaksi hipersensitivitas tipe 1 (type 1 hypersensitivity atau immediate-type hypersensitivity reactions)
Figure 12-2 Ke-4 Jenis Reaksi Hipersensitivitas alergi
Alergi Reaksi alergi terjadi bila individu yang sudahmempunyai antibodi IgE terhadap suatu antigen (alergen) tertentu (SUDAH TERSENSITISASI) terpapar pada alergen yang sama Antigen yang mengakibatkan alergi disebut alergen Alergen memicu aktivasi IgE yang terikat sel mast, mengakibatkan suatu rentetan kejadian yang disebut reaksi alergi
sensitisasi reaksi alergi
Figure A-24 Distribution of lymphocyte subpopulation in human peripheral blood 32
Subset limfosit BCD19+ T-helper CD3+ CD4+ T-cyt. CD3+ CD8+ 33