Download
1 / 19
190 likes | 331 Views
Adaptative designs and sites. Pierre Gervais President, Q&T Research, Sherbrooke President, AQRC. Discuss areas mostly affected with implementation of Adaptive Designs (AD). Approach to the patients, Remote data entry Study material. People Participants Nurses Physicians.

E N D
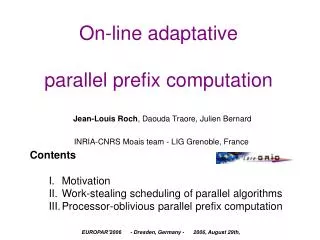
Adaptative designs and sites. Pierre Gervais President, Q&T Research, Sherbrooke President, AQRC
Discuss areas mostly affected with implementation of Adaptive Designs (AD) • Approach to the patients, • Remote data entry • Study material.
People Participants Nurses Physicians Systems Projects Work Finances Budget & Cash flow These changes are applied over an already rapidly changing environment Actual load of pressure on sites to make changes. What is changing?
Nurses • «Must have» qualities • Caring personality • Well integrated nursing and medical knowledge • Organised and structured mind… but also flexible • A «Make it Happen!» mentality • A «Sixth Sense» for problems • Bilingualism • Understanding roles and responsibilities • i.e. managing a study vs managing a site • CRO / Sponsor / Site management / PI / Auditor • Computer literate
Physicians • Dedicated research time • Clinical research set up that is changing from ‘’amateur’’ to ‘’professional’’ • Much more attractive ‘’Plan B’’ • More than 50% of physicians in the US will do only 1 trial. • Lack of US Investigators in ’08-’09 ?
Projects • Made on time • Increasing globalisation • Competitive pricing. • One ‘’case’’ in US = 1.0 $ • In Canada = 0.87 $ • In China = 0.18 $ • In India = 0.27$
Patients and population • General population has a • Negative opinion of drugs • Perceived guinea pig activity • Lack of trust • Negative press in general • Lack of knowledge of the population and the medical bodies
Perception is often that: • Drugs are commodities. • Drug companies are commodity providers.
Only in North America ? 4th Annual Forum on Patient Adherence, Compliance and Persistency November 29 - 30, 2007, Prague, Czech Republic • II. Are Patients Being Scared off Their Medicines?
There is a need to • Develop a sufficient level of confidence and support from the community. • By investigative sites • By pharmaceutical sponsors
AD / Approach to the patient • Sites must be very careful when explaining the details of clinical research, experimentation, side effects, risks, etc to patients. • Adaptative designs make our jobs even more challenging when we have to explain these complex designs and the risks of early treatment cessation are increased when designs are modified.
AD / Data entry • Sponsors must analyse early and rapidly • Data to be entered into the system as it is generated by the site • New role is allocated to the sites but unfortunately very often without the necessarily equivalent resources • data entry people • or specific budget for RDE
Actual management • Protocols of increasing complexity • More visits • More procedures • More documentation • SOP, archive, ‘’study binder’’, … • New roles, such as data entry (RDE) • More hidden costs: • SAE reporting, Amendment (s…), data lock, data queries, deadlines, etc • More reluctant patients
AD and management • All the above, plus • Complex study medication packages • Bulky laboratory boxes • Space is becoming an issue for centers • More reluctant patients
What’s next ? • Emergence of dedicated specialized in the conduct of trials • An increasing challenge • Part time investigative sites will not find their place with complex design and be left with much more simple trials, i.e. Phase IIIb and IV
What’s next ? • Many physicians may very well simply return to their clinic, a reaction that will further increase the lack of investigative physicians. More than 50% of US investigators will complete a 1572 only once.
In conclusion While the use of AD is increasing, sites have to adapt their work strategies and the skills of the research staff. … and to carefully adapt with these changes while maintaining high standards for work ethics.