Uveitis 3
180 likes | 700 Views
Uveitis 3. Dr. Mohammad Shehadeh. Introduction. Toxoplasmosis is caused by Toxoplasma gondii , an obligate intracellular protozoan . It is estimated to infest at least 10% of adults in northern temperate countries and more than half of adults in Mediterranean and tropical countries.

Uveitis 3
E N D
Presentation Transcript
Uveitis 3 Dr. Mohammad Shehadeh
Introduction • Toxoplasmosis is caused by Toxoplasmagondii, an obligate intracellular protozoan. • It is estimated to infest at least 10% of adults in northern temperate countries and more than half of adults in Mediterranean and tropical countries. • The cat is the definitive host and intermediate hosts include mice, livestock and humans
Mode of human infection • Ingestion of undercooked meat (lamb, pork, beef) containing bradyzoites of an intermediate host. • Ingestion of sporocysts following inadvertent contamination of hands when disposing of cat litter trays and then subsequent transfer on to food. Infants may also become infected by eating dirt (pica) containing sporocysts. It is likely that water contamination plays an important role in the transmission of the disease in rural areas. • Transplacental spread of the parasite (tachyzoite) can occur if a pregnant woman becomes infected.
Toxoplasmaretinitis • Toxoplasmosis is the most frequent cause of infectious retinitis in immunocompetent individuals. • Reactivation at previously inactive cyst-containing scars is the rule in the immunocompetent, although a small minority may represent new infection. • Recurrent episodes of inflammation are common and occur when the cysts rupture and release hundreds of tachyzoites into normal retinal cells. Recurrences usually take place between the ages of 10 and 35 years (average age 25 years).
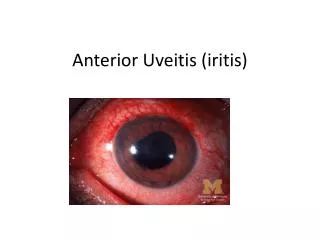
Clinical features • The diagnosis of toxoplasma retinitis is based on a compatible fundus lesion and positive serology for toxoplasmaantibodies • Presentation is with unilateral sudden onset of floaters, visual loss and photophobia.
Signs • ‘Spill-over’ anterior uveitis, which may be granulomatous • Solitary inflammatory focus near an old pigmented scar (‘satellite lesion’) • Multiple foci are uncommon • Severe vitritis may greatly impair visualization of the fundus, although the inflammatory focus may still be discernible (‘headlight in the fog’ appearance) (Fig. 11.24C).
healing • In uncompromised hosts healing occurs within 6 to 8 weeks (Fig. 11.25A-C) although vitreous opacities take longer to resolve. • The inflammatory focus is replaced by a sharply demarcated atrophic scar which becomes progressively pigmented starting at the edges, producing a hyperpigmentedborder. • Resolution of anterior uveitis is a reliable sign of posterior segment healing. • After the first attack, the mean recurrence rate within 3 years is about 50% and the average number of recurrent attacks per patient is 2.7
Fuchs uveitissyndrome • Fuchs uveitis syndrome (FUS) or Fuchs heterochromiciridocyclitis is a chronic non-granulomatous specific uveitis entity which is usually unilateral. • It has an insidious onset, occurs mostly in the 3rd–4th decades and affects both sexes equally. Although FUS accounts for about 4% of all cases of uveitis, it is frequently misdiagnosed and over-treated. • Theheterochromia(difference in iris colour between the two eyes) may be absent or difficult to detect, particularly in brown-eyed individuals
Presentation • Chronic, annoying vitreous floaters are often the presenting symptom. • Gradual blurring of vision secondary to cataract formation is common. • Colour difference between the two eyes. • Incidental detection.
General signs • Absence of posterior synechiae, except following cataract surgery. • KP are characteristically small, round or stellate and grey-white in colour. They are scattered throughout the corneal endothelium and are frequently associated with feathery fibrin filaments • Small nodules on the pupillary border and stroma (Fig) are seen in 30% of cases. • Aqueous humour shows faint flare and mild cellular reaction. • Vitritis and stringy opacities may be dense enough to reduce vision.
Heterochromiairidis is an important and common sign; it is demonstrated most effectively in daylight. • Most frequently the affected eye is hypochromic • In blue eyes, predominant stromal atrophy allows the posterior pigmented layer to show through and become the dominant pigmentation, so that the eye may become hyperchromic (reverse heterochromia).
Complications • Cataract is extremely common and is often the presenting feature (see Fig. 11.75E). It does not differ from that associated with other types of anterior uveitis. The results of surgery with posterior chamber intraocular lens implantation are good. • Glaucoma is a late manifestation which typically develops only after several years of follow-up. It is usually well-controlled on topical therapy, but some patients may require surgery.
Treatment is only indicated in patients with troublesome vitreous opacities. • Posterior sub-Tenon injections of a long-acting steroid preparation such as triamcinoloneacetonide may be beneficial although improvement is usually temporary. • Vitrectomy may be considered for severe vitreous opacification that is reducing vision or is very disturbing.
Lens-induced uveitis • Lens-induced uveitis is triggered by an immune response to lens proteins following rupture of the lens capsule, which may be due to trauma or incomplete cataract extraction • Phacoanaphylacticendophthalmitis: abrupt reduction in visual acuity and pain, days to weeks after rupture of the lens capsule by trauma or surgery: Tx by removal of the lens and steroids • Phacolytic glaucoma (PG) is the sudden onset of open-angle glaucoma caused by a leaking mature or hypermature (rarely immature) cataract. It is cured by cataract extraction.[1, 2, 3]