Download
1 / 49
490 likes | 495 Views
Prognostic value of occult breast cancer cells in blood and bone marrow. Gro Wiedswang Surgical unit, Ullevål University Hospital & The Micrometastasis lab, Radiumhospital-Rikshospital Oslo Norway. Rome 16.11.06. - why occult tumour cells - what is occult tumour cells

E N D
Prognostic value of occult breast cancer cells in blood and bone marrow Gro Wiedswang Surgical unit, Ullevål University Hospital & The Micrometastasis lab, Radiumhospital-Rikshospital Oslo Norway Rome 16.11.06
- why occult tumour cells - what is occult tumour cells - occult tumour cells in bone marrow - timing of bone marrow examination - occult tumour cells in blood - clinical trials - futher perspectives
Challenge of breast cancer • Better diagnostics • Screening • Improved surgical treatment • Improved adjuvant treatment 25-30% of N0 patients die whitin 5 years 40% of N1 patients survive > 10 år Overgaard NEJM 1997
Challenge of breast cancer • Therapeutic desicions • size of tumour • lymph node involvement • histological grade • hormone receptor • HER-2 status Improved prognostication! Feature of the patient??
Why micrometastasis? Cancer incidence: > 2500 women/year in Norway > 1mill women/ year wordwide Still 20% 5 year mortality in Norway Current treatment strategies does not catch patients at risk / overtreat low-risk patients Micrometastasis / occult tumour cells: - prognostic tool - identify high/low risk patients - monitoring therapy - identify therapeutic targets
Why micrometastasis ? Patients do relapse after removing the whole breast and negative lymph nodes Early, subclinical dissemination of tumour cells TNM staging does not catch all patients at risk Isolated tumour cells for prognostication ?
Mikrometastasis • Groups of tumour cells 0.2-2mm in another tissue than primary tumour (AJCC 2002, UICC 2002) • bone marrow / lymph nodes / blood • signs of invastion and organisation(Diel & Cote, Ca Treat Reviews 2000)
Occult tumour cells • disseminated tumour cells • circulating tumour cells • minimal residual disease • micrometastasis • early cancer spread
Pilot studies Relapse BM- 24% 25% 23% 15% Follow-up (mnd) 48 76 77 39 Ref. Salvadori 1990 Mansi 1991 Diel 1994 Harbeck 1994 BM+ 17% 25% 45% 38% Relapse BM+ 30% 48% 77% 39% p-value ns <0.005 <0.005 <0.005
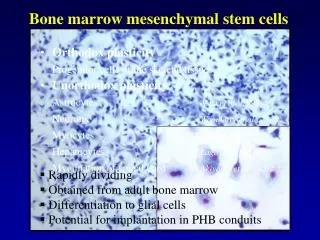
Oslo Micrometastasis project • Collaboration between several hospitals in the Oslo region • aspiration of 40 ml bone marrow from crista iliaca ant and post peroperatively • 920 patients included (1995-98)
Immunocytochemical detection • Single cell suspension2 x 106 cells/test • Spinns to slides • fixation - acetone • Anti-epitelial antibodyAE1/AE3 • Enzymatic visualisation of antibody -APAAP Y Y Y
Standardization of the immunocytochemical detection of cancer cells in BM and blood: I. Establishment of objective criteria for the evaluation of immunostained cells The European ISHAGE Working Group for Standardization of Tumor cell detection E. Borgen et al. 1999. Cytotherapy 1:377-388
Histopatological datan=920 frequency Nodal status Tumor status N0 N+ T1 T2 T3-4 63% 33% 58% 29% 6% Naume et al Clin Can Res 2001;7:4122-9
Detection of tumour cells BM+ Tumourstatus T1 11.2% T2 15.0% T3 22.6% N0 9.9% N+ 20.6% Nodalstatus Naume et al Clin Can Res 2001;7:4122-9
Correlation of bone marrow positvity to other known prognostic characteristica 0.055 0.128 0.575 0.024 0.045 BM+ p-value ER/PgR p53 Catepsin D c-erbB2 Vascular infiltration 12.0 % 17.6 % 16.2 % 11.9 % 13.1 % 14.6 % 23.9 % 12.3 % 17.4 % 12.6 % +/-,-/+,+/+ -/- Pos Neg Pos Neg Pos Neg Yes No Naume et al Clin Can Res 2001;7:4122-9
Clinical follow-up No of patients with infiltrating cancer, M0 and evaluable immunocytology Obs.time median (range) No of relapses No of systemic relapses No of locoregional relapses No died of breast cancer 817 49 (½-85) mnd 174 (21%) 127 (16%) 47 (6%) 94 (11%) Wiedswang JCO, 18; 3469, 2003
Localisation of systemic relapse Frequency % Skeleton Liver Lung CNS 10.2 5.8 5.2 1.9 Wiedswang JCO, 18; 3469, 2003
Survival according to bone marrow status DDFS BCSS BM- BM- BM+ BM+ p<0.001 p<0.001
Survival lymph node-pos (N+) DDFS BCSS BM- BM- BM+ BM+ p=0.001 p=0.008
Survival lymph node-negative (N0) BCSS DDFS
Survival T1N0 without adjuvant treatment p=0.014 P<0.001
Uni -& multivariat analysis • Cox-regression: • BM+ versus BM- • histological grade • T1 versus T2-4 • N0 versus N1 • hormone receptor (ER+ or/and PgR+ versus both-) • p53 • c-erbB2 • catepsinD • vascular infiltration
Multivariat analysis(Cox regression)p -values breast cancer specific survival All N+ N0 T-status <0.001 <0.001 ns N-status <0.001 BM 0.018 0.015 ns hormonreceptor <0.001 <0.001 ns histologic grade 0.002 0.017 0.021
Multifactorial survial analyses with BM status BM- BM- BM+ BM+ P<0.001 p=0.003
Mansi et al Patient inclusion: 1981-86 Mansi et al. 1987/91/99
Occult tumour cells in bone marrow and clinical outcome Braun et al, 2000, NEJM
Persisting tumor cells in BM after chemotherapy - the impact on survival Braun et al. 2000
Second bone marrow aspiration 3 years after surgery • Pasient characteristics (n=356) • 70.2% T1 • 71.9% N0 • 80.1% hormon receptor positiv • 14.9% BM+ • correlates to nodal status and adjuvant treatment
Second bone marrow aspiration 3 years after surgery • Clinical data: • 26 mnd after BM2 • 66 mnd after primary surgery • 32 relapses • 12 local • 20 systemic • 10 pasients died of breast cancer
Survival according to second bone marrow status Distant disease free survival Breast cancer spesific survival p<0.001 p<0.001 Wiedswang et al Clin Ca Res 2004
Breast cancer specific survival N0 (n=256) N+ (n=93) p=0.003 p=ns Wiedswang et al Clin Ca Res 2004
BM1 & BM2 • n= 356 patients • 4 groups: ++ 17 patients +- 54 ” -+ 33 ” -- 231 ”
BM1 & BM2 Breast cancer specific survival Distant disease free survival ++ ++ p<0.001 p<0.001 Wiedswang et al Clin Ca Res 2004
Occult tumour cells in blood and bone marrow, correlated to clinical outcome (n=341) DFS DDFS BCSS BM- BM- BM- BM+ BM+ BM BM+ Cumulative survival Events/total no of pts: BM-: 8/293 BM+: 6/48 Events/total no of pts: BM-: 17/293 BM+: 10/48 Events/total no of pts: BM-: 23/293 BM+: 14/48 p<0.001 p<0.001 p=0.001 PB- PB- PB- PB+ PB+ PB+ PB Cumulative survival Events/total no of pts: PB-: 8/307 PB+: 6/34 Events/total no of pts: PB-: 28/307 PB+: 9/34 Events/total no of pts: PB-: 20/307 PB+: 7/34 p=0.001 p=0.002 p<0.001 Months after operation Wiedswang et al Int J Ca 2006
Benoy et al Br J Ca 2006 RT-PCR BM and blood 147 M0/M+ pts Bone marrow superior to blood in predicting outcome