Download
1 / 21
210 likes | 585 Views
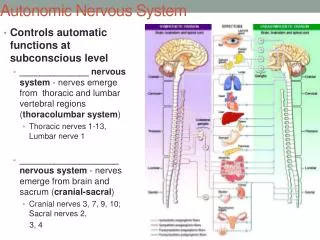
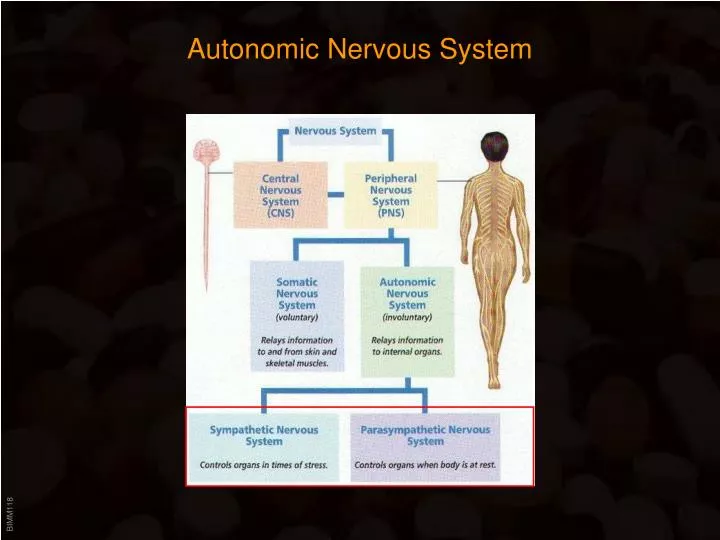
Autonomic Nervous System. Autonomic Nervous System. Ganglia close to the innervated organs Myelinated axons. Ganglia close to the spinal column Preganglionic axons are myelinated; postganglionic axons are unmyelinated . Note : Somatic nervous system has no ganglia!.

E N D
Autonomic Nervous System • Ganglia close to the innervated organs • Myelinated axons • Ganglia close to the spinal column • Preganglionic axons are myelinated; postganglionic axons are unmyelinated • Note:Somatic nervous system has no ganglia!
Autonomic Nervous System Transmitters: • Acetylcholine: • ALL preganglionic neurons • ALL parasympathetic postganglionic neurons • Norepinephrine (= Noradrenalin): • MOST sympathetic postganglionic neurons • Exceptions: Sweat glands (Acetylcholine); Renal arteries (Dopamine) • Epinephrine (= Adrenalin): • Adrenal medulla upon sympathetic impulses (no ganglion!)
Adrenergic System Termination of (nor)epinephrine action: • Reuptake into presynaptic nerve ending • Predominant mechanism • active transport; inhibited by Cocaine • Catechol-O-methyltransferase (COMT) • In the cytoplasm of post-junctional cells • Monoamino-oxidase (MAO) • In mitochondria of nerve and post-junctional cells • Presynaptic a2-receptors • Negative feedback that inhibits norepinephrine release
Adrenergic System Adrenergic receptors: • alpha 1 • most vascular smooth muscles • Activate PLCb => Ca++ => Contraction • alpha 2 • mostly presynaptic • Inhibit adenylate cyclase (Gai) • beta 1 • mostly heart • Activate adenylate cyclase • beta 2 • respiratory and uterine smooth muscle • Activate adenylate cyclase • beta 3 • mostly adipocytes • Activate adenylate cyclase => lipolysis • (Dopamine)
Adrenergic System - Agonists Sympathomimetics Indirect Sympathicomimetics: MAO - Inhibitors: • Inhibition of MAO causes increase in free Norepinephrine • In the CNS, MAO also metabolizes dopamine and serotonin => MAO inhibitors trigger increase in these “happy hormones” => uses as antidepressants • Irreversible inhibition of MAO => long-lasting effect (weeks!) • Tranylcypromine • Moclobemide Possibility of severe adverse interactions of MAO inhibitors with numerous other drugs => fatal hypertension
Adrenergic System - Agonists Epinephrine Ephidrine Sympathomimetics Indirect Sympathicomimetics : • Ephedrine • Chief alkaloid in Ephedra, no clinical use • Displase norepinephrine in storage vesicle => forced norepinephrine release • Found in many dietary supplements: “Energy-Boosters”, Diet pills (Metabolife®) etc. • Ingredient in many herbal preperations:Ephedra, Ma Huang The FDA has received more than 800 reports of adverse effects associated with use of products containing ephedrine alkaloid since 1994. These serious adverse effects, include hypertension (elevated blood pressure), palpitations (rapid heart rate), neurophathy (nerve damage), myopathy (muscle injury), psychosis, stroke, memory loss, heart rate irregularities, insomnia, nervousness, tremors, seizures, heart attacks, and death. On April 12th, the agency has banned the marketing of dietary supplements containing ephedrine alkaloids.
Adrenergic System - Agonists Sympathomimetics Indirect Sympathicomimetics : Amphetamines • Displace norepinephrine in storage vesicle => forced epinephrine release • Also inhibit norepinephrine re-uptake and degradation by MAO (“triple action”) • Methylphenidate (Ritalin®) • Treatment of ADD • Fenfluramine • Appetite suppressant (now banned in US)(combined with Phentermine = “FenPhen”) • Metamphetamine/MDMA • Effectiveness disappears due to norepinephrine depletion of vesicles => post-use depression => urge for re-administration!
Adrenergic System - Agonists Sympathomimetics Non-selective agonists: • Epinephrine (Adrenaline) • Activates both a and b receptors; • Blood pressure increase, but effect on systolic pressure dominant • Dilates bronchii • Potent vasopressor => Clinical uses limited • Used for: symptomatic treatment of anaphylactic shock (Epi-Pen®)adjuvant in local anesthetics (increases duration, reduces bleeding) • Norepinephrine (Noradrenaline) • Activates mostly a receptors => systolic and diastolic blood pressure increase • Very potent vasopressor => Clinical uses limited to severe shock treatment
Adrenergic System - Agonists Sympathomimetics a1 - selective agonists Clinical applications: • Methoxamine • Treatment of hypotensive state • Phenylephrine • (Local) vasoconstrictor nasal decongestant Epinephrine Phenylephrine
Adrenergic System - Agonists Sympathomimetics a1 - selective agonists (cont’d) Clinical applications: Nasal decongestants (mostly OTC): • Naphazoline (Privine®, Rhinon®) • Oxymetazoline (Afrin®, etc.) • Xylometazoline (Privin®) Should be used less than 10 days, otherwise reactive hyperemia (“rhinitis medicamentosa”) develops! Continued used can result in local hypoxia => atrophic damage of the nasal mucosa
Adrenergic System - Agonists Sympathomimetics a2 - selective agonists Phenotypically produce sympatholytic effects! Inhibit presynaptic a2 receptors in the cardiovascular control center in the CNS => reduced sympathetic nervous system activity => blood pressure decrease Clinical applications: Hypertension • Clonidine • Guanfacine
Adrenergic System - Agonists b1 - receptors • Mostly in heart • Increase contractility = “positive inotrope” • Increase heart rate = “positive chronotrope” b2 - receptors • Respiratory system – located in bronchial smooth muscle • Produce bronchial dilation
Adrenergic System - Agonists Sympathomimetics b1 - selective agonists Clinical applications: • Dobutamine • Strong inotropic effect with little chronotropic effect =>increase in cardiac output without significant increase in heart rate • Short-term treatment of impaired cardiac function after cardiac surgery, MI etc. • Also used in “Dobutamine Stress Test” = Heart sonogram: Dobutamine mimics exercise Epinephrine Dobutamine
Adrenergic System - Agonists Sympathomimetics b2 - selective agonists Clinical applications: Asthma: • Non-selective sympathomimetics => strong cardiac side effects • b2 - selective agonists target predominantly the respiratory system • Drugs differ in speed of onset and in duration of action => acute vs. long-term treatment • Additionally, preferential activation of pulmonary receptors due to application as aerosols • Metaproterenol (Alupent®) • Albuterol = Salbutamol (Ventolin®) • Formoterol (Foradil®) • Etc…
Adrenergic System - Antagonists Sympatholytics a - selective antagonists Promote vasodilation => decreased peripheral resistance => blood pressure (Side effects: reflex tachycardia and postural hypotension) Relaxation of the smooth muscles in the bladder neck Clinical applications: Hypertension; Urinary retention Non-selective a-antagonist: • Phentolamine (for pheochromocytoma) • Ergot alkaloids see HT-5 receptor a1 -selective antagonists: • Prazosin(Minipress®) first a1 - selective antagonist • Terazosinlonger half-life • Doxazosinlonger half-life
Adrenergic System - Antagonists Sympatholytics a2 - selective antagonists • Yohimbine • Chief active compound in Pausinystalia yohimbine (bark) • Effects opposite of Clonidine • Enters CNS => increased sympathetic output => increased heart rate, blood pressure, can cause severe tremors • Ingredient in many weight loss products • Extensive (past) use in treatment of male sexual dysfunction
Adrenergic System - Antagonists Sympatholytics b - selective antagonists (”b - blockers”) b2 - selective antagonistswould trigger bronchial constriction => no clinical use b2 - antagonism is mostly an “undesired side effect” of b-selective antagonists (goal is to antagonize b1 - receptors) Non-cardiac effects: CNS - anxiolytic; skeletal muscle - reduction of tremor Clinical applications: • Angina pectoris • Hypertension • Cardiac dysrhythmias • MI • Heart failure • Familial tremor • “Stage fright”
Adrenergic System - Antagonists Sympatholytics b - selective antagonists • First-generation b-receptor antagonistsblocked b1 and b2-receptors = noncardioselective (b-receptors in the heart are b1 - receptors). • Manyb-receptor antagonistsposses intrinsic agonist activity • Basic conserved structure: Norepinephrine side chain linked to aromatic structure by a methylene-oxygen bridge. Prototype: • Propranolol Epinephrine
Adrenergic System - Antagonists Sympatholytics b - selective, noncardioselective antagonists (cont’d): • Nadolol • Pindolol • Timolol • Labetalol- also antagonistic on a1 - receptors => potent antihypertonic drug b1 - specific “cardioselective” antagonists: • Metoprolol • Atenolol • Esmolol- quick onset / short duration => used in urgent settings
Adrenergic System - Antagonists b-Sympatholytics Epinephrine