Download
1 / 10
100 likes | 219 Views
Successful allogeneic SCT in infant with FHL, dilemmas in using „unaffected“ sibling. P.Sedláček, R. Špíšek, et al 2nd Medical School, Charles University, Prague, CZ. ESID – May 10.-11. 2004. Past Medical History (family). mother HBsAg +, no transf.history father – OK

E N D
Successful allogeneic SCT in infant with FHL, dilemmas in using „unaffected“ sibling P.Sedláček, R. Špíšek, et al 2nd Medical School, Charles University, Prague, CZ ESID – May 10.-11. 2004
Past Medical History (family) • mother HBsAg +, no transf.history • father – OK 1st girl – died 32nd gest.week (umb. cord problems) 2nd boy (IVF) – Jakub – alive/well 3rd girl (IVF) - Jana * July 8th 2003
History of Present Illness I – early postnatal pancytopenia (WBC : 4,8, RBC: 3,1, ret.: 0,1%, ANC: <100, Plt 11) allo HLA Ab in mother exchange transfusion (D+9), PRBC, Plt, Fbg HSmegaly, hepatopathy, hypertriglycemia, hyperbilirubinemia hyperferritinemia ( >18 000) DIC, infections, fever and elev. CRP, HBsAg and HBeAg negative (Engerix, Hepatect) Admission to our department at the age of 28 days (Aug.2003)
History of Present Illness II • Day of admission Aug. 5th 2003 • liver +4cm, spleen +3-4cm bcm, pancytopenia • Therapy according to HLH 94 • (VP16, Dexa, CsA) • discontinued for acute sepsis • Transfusion history pre SCT • PRBC 13 x (or more) • Plt more than 13
Pre-transplant condition • HSmegaly, ferritin 3153 • antiHBc and antiHBe pos., HBsAg neg. • Failure to thrive (bw 3,45 kg; 2,8 kg at birth) • normal LFT; Plt 100, WBC and RBC normal • brother fully HLA matched, 19kg bw, 3yo • ABO incompat. : A+ vs. B- (low titers)
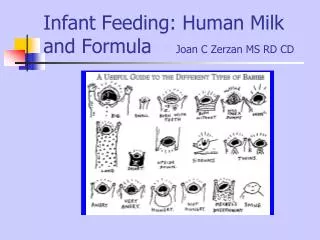
Control Control Brother´s NK cells Patient´s NK cells Diagnostics-1 FACS analysis of perforin expression in NK cells Exclusion of FHL type 2- perforin deficiency 87% of NK cells are perforin + 87% of NK cells are perforin +
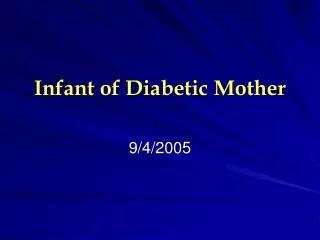
control brother % cytotoxicity • defective cytotoxic activity of patient´s lymphoblasts • normal findings in her brother donor of SC X patient Diagnostics-2 • Cytotoxic activity of T-lymphoblasts generated from T-cells • Target cells: L1210 cells deficient in FAS expression
Transplantation • 11.9.2003 (* 8.7.2003) • Bu(19mgkg) + Cy(200) + rATG(25mg/kg) • CsA + MP (MTX not used due to early and severe VOD) • BM : NC : 8,9x 108/kg; CD34: 22x106/kg • VOD : D+1 (D-3 through D+15 defibrotide) • Bilirubinemia, thrombocytopenia, ascites, ARDS • Engraftment :ANC (500) D+19; Plt (20/50) D+22/+26 • Chimer. : stable, 95% donor • Discharched to outpatient clinic D+34 • no aGVHD, no cGVHD so far (~D+240) • continues on CsA, steroids D/C ~D+50 • growth catch-up
Acknowledgement • Department of Pediatric Hematology and Oncology • HSCT unit; Division of Hematology • Institute of Immunology • diagnostics of primary HLH • Institute of Hematology and Blood Transfusion • HLA typing