Download

1 / 53
530 likes | 652 Views
ms. Principles and values of effective team-based health care Example: TBC and improving hypertension control Challenges to teamwork in clinical care What does "leadership" mean in a high-functioning team? What might a "trans-disciplinar y " professionalism look like?.

E N D
ms • Principlesandvaluesofeffectiveteam-basedhealthcare • Example: TBCandimprovinghypertensioncontrol • Challengestoteamworkinclinicalcare • Whatdoes"leadership"meaninahigh-functioningteam? • Whatmighta"trans-disciplinary"professionalismlooklike?
DisclosureandDisclaimer • Disclosure • Ihavenopersonalfinancialrelationshipswithanypharmaceuticalcompaniesandnoneofmyworkis fundedbypharmaceuticalcompanies. • TheAMAreceivessomedirectsupportforotherprojectsandprogramsfromfor-profitcompanies(<15%oftotalAMAbudget). • Disclaimer • Theviewsexpressedinthispresentationaremyown. • NothingIsayshouldbe construedasrepresentingapolicyoftheAMA, unlessIspecificallysayotherwise. . -L'i I , .' • I . - 1.....
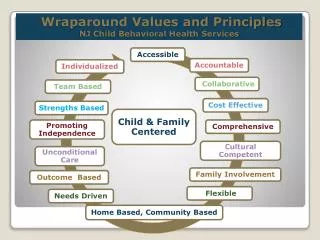
SharedGoals... Worktoestablishsharedgoalsthatreflectpatientandfamilyprioritiesandthatcanbeclearlyarticulated,understood,and supportedbyallmembers.
Clear Roles... Haveclearexpectationsforeach member'sfunctions,responsibilities, andaccountabilities.
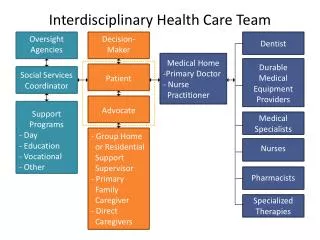
Patientsandfamiliesasmembersofteams, • ratherthanrecipientsofteamcare • Leadershipinthecontextofteam-basedcare • Teachingandtrainingforteam-basedcare • "External"factorsthatsupportorhindereffectiveteam-basedcare(organizational,systemic,financing,legal,etc.)
PreventableDeathsfromHeartDisease&Stroke CardiovasculardiseaseandtypeIIDiabetes
+Diseasesandinjuries +Riskfactors • Highbloodp12Ssure 7 + Smoking- 6 +Alcoholuse +IHD s +LRI DietlowinFruit • + HAP + Cerebrovasrulardisease 4 l.Dwbadpain I • HighBMI • +FPG Malaria +Diarrhoea. ++Hr/COPD • ........_+Roadinjuiy++PMHAmb 3 / .......... •lnactivityt PretbirthUndefweight+Sah comphcabonS •, +Dietlowinnutsandseeds 2 • -Tuberculosis Diabetes + Lungcancer 1 10 Deaths() 16 20 1 1 14 ffgt.re2:CompartsonofthemagnJtudeoftheten leadlngdlseasesandlnJur1esandthetenleadlngr1skfactorsbasedonthepercentageofglobaldeathsandthepercentageofglobalDALYs,2010 actors orpooreat 2010 1990 I1Childhoodunderweight 1Highbloodpressure2Tobaccosmoking,excludingsecond-handsmoke3Alcoholuse "14Householdairpollutionfromsolidfuels 1Lowerrespiratoryinfections 2Diarrhoea3Pretermbirthcomplications 4lschaemicheartdisease 1lschaemicheartdisease ·I2Lowerrespiratoryinfections 3Stroke '14[)iarrhoea I2Householdairpollutionfromsolidfuels 3Tobaccosmoking,excludingsecond-handsmoke4 Hihbloodpressure IsHIV/AIDS ISSuboptimalbreastfeeding ISDietlowinfruits -Ascendingorderinrank Communicable,maternal,neonatal,andnutritionaldisorders
3ImprovementConcepts • MeasureAccurately • ActRapidly • PartnerwithPatients • &Families
Team-BasedCareisaPotentAnti-hypertensive • • • I -14.0 l-'ac1l11.a1ed1-'iment!-'anent Aud11&TeamChange All Pro\•1derl'rov1dercompamonseducation(11)reminder(6)(adjusccdfor stud)size& Difl'Prc:N33) All compansons(unadjusicd, t\=33) Self- relayofex:lucanon(18)managementremmdersI5)feedhock(3) (20) infollllation (16) (9) Quality Improvementtrategy "InterventionsthatincludedteamchangeasaQIstrategywereassociatedwiththelargestreductionsinbloodpressureoutcomes.Allteamchangestudiedincludedassignmentofsomeresponsibilitiestoahealthprofessionalotherthanthepatient'sphysician." Walshetal2006;ArchInternMed
CochraneReview,2010 MeJO Me;inC>iffefma! IVJ1>;ed.95%0 St °'Slbzl"CX.'P Waz Dffermce IV;R>af,95%Cl Tre.:itrnent N 1"..'e:1.:('SO) Control N n(SD) 21% -1200(-2057,143] Bogden 1998 49 -23(226) 30 .(,(14.7) 345 6.8(17.4) 349 -2(14..1) 23 -123(1511) IIO-<..I(15.7) 63 -&2(15.1) 118ll3(17.l) 48 -24(116) 29 -10(8.7) 46 -11(20) 34 -I (14.J) 338 3.5(17) 280 -2(10.7) 170.7 (18.B) oeCls:m1006 3.1% -5..00(-1213,2131 • ll4% -3.D(5.88,-On] GartiJ-R?n:i. 200I H:r.\.1<;79 P.:lric199(, 41.4% 0.0[-1.94,1.941 1.7% -13.00[-2259,-1411 -1.70[6..4J.,102i 6..90[-127J.,-1.08] s.roc-10.1a-1.111 -7.00(-13.45,-0.55] ...(18.3) 7.0% '94 Schroeder2005 -1.3(19) 4.l.% Sdonxx2001 70 • 117 -176(IB.l.) 7.4 % Soobnein! 2004 -17(18.1) 3.7% 47 Tobe2006 Ton2007 18 5...5 % 0.0[-S3Q5JO1 -10 -1) Total(95%CI) HeteroCtt:? 1164 23.46.df 9(P =0.0I 100.0% -2.52[-3.77,-1.27] 1071 P.?=62% lestforO\oer.ieffettZ=3.96(P=01Xl0075) Testfocsubf;rc:x:i:>cfr!fcrmces:Not;!ppral:ie
Overcometherapeuticinertia • Improveadherencetoevidence-basedguidelines • Streamlinedcareprocesses • Teamsgiveexplicitthoughtto processissues • Increased'dose'ofhealthinformation/advice • Morepointsof contact • Moretimespentwithhealthprofessionals • Additionaltypesofinformationprovided • Betterinterpersonalconnectionswithpatients
Therearealwaystensionsthatcomeup.Partofworkingis dealingwithtensions.Ifthere'snotension,thenyou'renotseriousaboutwhatyou'redoing. WyntonMarsalis
Hot Button Terms • Scope of practice • Independentpractice • Supervision • Physician-led • Doctor • Mid-level • Allied health • Collaboration
...thenuancednatureof"Leadership"withinteamscarryingoutcomplexorinnovativework...[requires]Leadershipfromallmembersoftheteam......thenuancednatureof"Leadership"withinteamscarryingoutcomplexorinnovativework...[requires]Leadershipfromallmembersoftheteam... "Physician-Led"Teams Leadershipisnot a clinical skill
LeadershipinTeams • TechnicalProblems • Problemisclear • Expert/leaderprovidessolution • Solutionseasytoaccept • AdaptiveChallenges • Problemhardtoacknowledge • Theteammustprovidethesolution • Solutionrequiresdifficultchange
Themostcommonfailurein leadership isproducedbytreatingadaptivechallengesasiftheyweretechnical problems Ronald Heifetz, Marty Linsky & Alexander Grashow, The Practice of Adaptive Leadership: Tools and Tactics for Changing Your Organization and the World (Boston: Harvard Business Press, 2009), 19; 23-24.
TRIP/CUSP Models Educatestaffonscienceofsafety 1.Summarizetheevidence inabehavioralchecklist MeasureAccurately ActRapidly Support PatientsandTheirFamilies 1. 2. Identifydefects 2.Identifylocalbarrierstoimplementation Assignexecutivetoadoptunit 3. 3.Measureperformance Learn fromonedefectperquarter 4. Ensureallpatients get theevidence Implement teamworktools • Engage • Educate • Execute • Evaluate
...Thedangerofanycaremodelinwhichthecaregiverisbroadlyconceivedasateamratherthanasan individualisthepossibledilutionofresponsibilityassumedbyindividual caregivers.Withoutsafeguards,noindividualmemberoftheteammayfeelcompelledtogotheextramiletoensurethedeliveryofnecessarycare. ...Giventhebreadthofprimarycare,licensureandregulationcannotrestrainnonphysicianprimarycaregiversfromofferingprimarycareservicesthattheyarenotqualifiedtoprovide. Onlyprofessionalismwillkeepsuch caregiversoperatingwithintheirsphereofcompetence-asisthecaseforall clinicians,includingprimarycarephysicians. Tom Huddle, Annals of Internal M ed icine, September 2013
Profess ProfessionProfessionalProfessionalism Definitions Unidisciplinary -OnegroupworkingaloneMultidisciplinary-Multiplegroupsworkingindividuallyonasharedissue Interdisciplinary-Multiplegroupsworkingtogethertowardacommongoal(AKA"interprofessional")Transdisciplinary-Multiplegroupsworkingtogether todevelopanew,sharedmodeland commonlanguage
"Transdisciplinaryprofessionalismcouldbedefinedas'an approachtocreatingandcarryingoutasharedsocialcontractthatensuresmultiplehealthdisciplines,workinginconcert,areworthy ofthetrustofpatientsandthe publicinordertoimprove thehealthofpatientsandtheircommunities.'" InstituteofMedicineoftheNationalAcademyofSciencesGlobalForumonInnovationinHealthProfessional Education
ANew,SharedSocialContract • Socialcontractsspellouttherelationsbetweenindividuals, • groupsandsociety • Gaincoherence,smoothfunction, reliability,safety... • ...attheexpenseofsome individualliberty(agreetoplaybytherules)