Download
1 / 32
320 likes | 505 Views
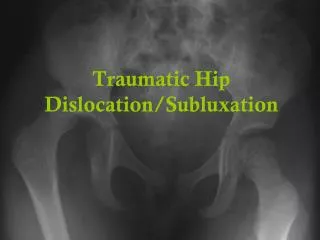
Traumatic conditions of the hip. Dislocation of the hip. Anterior dislocation Posterior dislocation, more common Central dislocation (direct thrust along the line of the femoral neck → fracture acetabulum → femoral head displaced into the pelvic cavity. Posterior dislocation of the hip.

E N D
Dislocation of the hip • Anterior dislocation • Posterior dislocation, more common • Central dislocation (direct thrust along the line of the femoral neck → fracture acetabulum → femoral head displaced into the pelvic cavity
Posterior dislocation of the hip • Longitudinal thrust along shaft of femur when hip is flexed & adducted (dash board accident) → head of femur displaced backward out of the acetabulum • Clinically: The affected leg is: • Internally rotated • Adducted • Shortened (fig.)
Complications • Immediate complications: Sciatic nerve injury → drop foot & numbness over the outside of the calf • Late complications: avulsion of ligamentum teres from the acetabulum → cut off blood supply to femoral head → avascular necrosis → OA
TREATMENT • Manipulative reduction • Traction (4 weeks) → healing of capsular tear • Weight bearing • Regular x rays monthly for the 1st 4 months for early detection of avascular necrosis
Treatment of complications • Operation may be necessary to free the sciatic nerve • Avascular necrosis is treated • in early stages by avoidance of WT bearing until texture of femoral head returns to normal. • In late stages by total hip replacement, arthrodesis, osteotomy, or bone grafting
Anterior dislocation of the hip • Force that abducts the extended hip → femoral head displaced below & in front of the acetabulum • Clinically: the affected leg is: • Abducted • Externally rotated • Treatment: • Manipulative reduction • 3 weeks traction
Central dislocation of the hip • Direct violence → drives femoral head through floor of acetabulum → • Damage of articular surfaces • Intrapelvic haemorrhage • Hypovolemic shock • Conservative treatment • Longitudinal traction for 6 weeks • Mobility of the hip • Surgical treatment • Reconstruction of the destroyed acetabulum • Total hip replacement
Fractures of upper end of femur • Risk factore: • Age: risk doubles over age of 50 • Sex: women > men 2-3 times • Race: caucasian > negroes 2-3 times • Medical history of previous hip fracture
Subcapital fracture of the femoral neck • Grade I Head of femur is abducted & impacted with the neck • Clinically: • Little pain • Trivial injury • No shortening or rotational deformity • Active movement may be possible
Grade II Undisplaced fracture ST are attached providing blood supply • Grade III • Femur is adducted at fracture site • Head is separated from the neck • Severe pain in hip when standing or moving the affected limb • Injured foot & leg are externally rotated
Grade IVGross rotation of both fragments with complete loss of contact between the fragments
Treatment • Grade II → - compression screws 2. Grade III & IV → • hemiarthroplasty (Austin-more prosthesis) • Total hip replacement
Intertrochanteric fractures • Common in elderly people • Equal frequency in men & women • Often comminuted • Lesser trochanter frequently avulsed & pulled upwards by iliopsoas • Treatment • Compressiom screws and plate • Early mobilization • Early ambulation
Fractures of femoral shafts in adults • Vigorous trauma • Hypovolaemic shock • Fracture line is transverse or comminuted • Severe displacement • residual stiffness of knee • Non-union with open fractures
Conservative treatment • Temporary traction for 8 weeks (fixed or balanced- skin or skeletal) (fig.) • Followed by hinged cast brace • Weight bearing is then encouraged Operative treatment • Locked intramedullary nail
Femoral shaft fractures in infancy • Causes: • Indirect rotatory twisting strain • Difficult delivery with breech presentation • Treatment: • 3-4 weeks fixed traction on Thomas splint • In infants less than 3 years → gallows traction
Supracondylar fractures • Treated by Thomas splint with knee flexion Fractures of femoral condyles • Intra-articular fracture • Internal fixation with plate and screws is necessry to: • Reduce the fractured articular surfaces accurately • Allow early mobilization
Physical therapy program during immobilization period • To prevent respiratory complications → breathing exercises. • To prevent circulatory complications → - circulatory exercises - changing position every 2 hours - alternating air mattress 3. To prevent stiffness, weakness & atrophy of the free parts → - ROM exercises - strengthening exercises 4. To prevent weakness of immobilized parts → static & isometric exercises
Rehabilitation after ORIF of hip fractures • Bed mobility while maintaining proper alignment of the operative limb • Lying flat on back for 1 hour/day to avoid hip flexion contractures. • Forced hip flexion or rotation (e.g. twisting forward or to either side)is to be avoided for the 1st 7-10 days postoperatively. • Patients are allowed to assume a semireclined position after 24 houurs.
5. Patients are assisted into protectively positioned side-lying as soon as possible(2-3 days postoperatively). • Side lying position greatly aids in: - toiletry - pulmonary postural drainage - prevention of decubitus ulcers 6. An over head trapeze is essential during the 1st few days postoperatively (using elbows & heels to elevate hips→ 4 times body weight force acts on the hip).
7. Gait training with walker or crutches if balance & mobility are good. (touch down gait takes about 90-95% of load off hip joint, compared to 80% weight reduction with NWB gait 8. Over 12-16 weeks gait pattern will evolve into full weight bearing based on: - surgical procedure - area of fracture - radiographic findings - patient comfort
9. Active exercises through a comfortable range 10. Pool exercises to regain strength, proprioceptive sense & mobility. Nb. • Tying a shoe with foot on floor requires 124o hip flexion • Ascending stairs requires 67o hip flexion • Sitting down on a chair requires 104o hip flexion
Fractures of upper end of femur(ORIF) Day 1: • Quadriceps sets • hamstrings sets • gluteal sets • ankle pumps
Active assisted hip abduction & adduction • Supine leg slides for flexion of hip & knee • Upper extremity exercise
Day 2: • Ambulation with TDWB with walker, then PWB with walker Days 3-7 • SLR in all directions • Thomas stretch of anterior capsule and hip flexors
1-2 weeks • Discharge criteria: • Get out of bed independently • Able to ambulate 50 feet with assistive device • In & out of bathroom independently. • Standing hip abduction, adduction, flexion, and extension & hip and knee flexion exercises. 2 -6 weeks • Stationary bicycle, pool exercises, and treadmill • Progress ambulation from walker to use of a cane (if Trendelendburg test is –ve)
Femoral shaft fracture treated with intramedullary nail • Phase 1: 0-6 weeks: • Quadriceps, hamstrings, gluteal sets & ankle pumps • SLR in all planes • Knee active ROM exercises • Stationary bicycle • Weight bearing to tolerance (if nail diameter is 12mm or more) an progress to full weight bearing as tolerated within 6-12 weeks. If nail diameter is less, begin weight bearing with 25kg.
Phase 2 (6 weeks -3 months) • Scale technique for weight bearing (5-10 kg increase weekly) • Isokinetic exercises • CKC exercises Phase 3 (3-6 months) • Full weight bearing • Full knee & hip ROM • Full squat • Ascend & descend stairs full weight bearing • Thigh circumference = uninjured side Phase 4 (> 6 months) • Return to athletic activity • Full work & recreational activity
Femoral shaft fracture treated with plate & screws • Same as for intra-medullary nail with exception that: • NWB for 8-12 weeks • Weight bearing is not progressed until radiological union (3-6 months)
Intraarticular fractures with IF • Phase 1 (0-6 weeks) • CPM in first 24-48 hours (0-90 degrees) • OKC exercise e.g. SLR, quadriceps sets • TDWB Phase 2 (6-12 weeks) • Stationary bicycle • PWB using the scale technique • CKC exercises
Phase 3 (3-6 months) • FWB Phase 4 (>6 months) • Return to work & recreational activity • Avoid excessive squatting & jumping & contact sports for 6-12 months