Download
1 / 53
630 likes | 1.32k Views
Colon & Rectum Injuries. Prayuth Sirivongs M.D. COLONIC INJURIES. Anatomy Cecum Ascending colon Transverse colon Descending colon Sigmoid colon. Etiology Penetrating Injury : Gun Shot ~ 75% Stab wound ~ 20% Blunt Injury : Motor vihicle

E N D
Colon & Rectum Injuries Prayuth Sirivongs M.D.
COLONIC INJURIES Anatomy • Cecum • Ascending colon • Transverse colon • Descending colon • Sigmoid colon
Etiology Penetrating Injury : Gun Shot ~ 75% Stab wound ~ 20% Blunt Injury :Motor vihicle Trananal Injury : Iatrogenic ; colonoscopy ,B.E. Sexual related : foreign body COLONIC INJURIES
Diagnosis Pre-operation Blood in rectum Acute abdomen series Water soluble contrast enema Triple contrast CT COLONIC INJURIES
COLONIC INJURIES Intra operation Rule of “ two “ Complete mobilize Blood staining Fecal odorsegmental squeeze
Treatment Colostomy Exteriorized repair primary repair COLONIC INJURIES
colostomy End Colostomy Protective Colostomy COLONIC INJURIES
colostomy End Colostomy Protective Colostomy COLONIC INJURIES
Indication for colostomy ( Stone & Fabian) 1.Shock c BP<80/60 mmHg 2.Intraperitoneal blood loss > 1000 ml 3.Intra-abdominal organ injuries > 2 organs 4.Significant fecal contamination 5.Time to operation >8 hrs 6.Colonic wound require resection 7.Major loss abdominal wall /Mesh COLONIC INJURIES
Colonic Injury Severity score(Shanon&Moore) Grade 1 ; Serosal injury Grade 2 ; Single wall injury Grade 3 ; < 25% wall involvement Grade 4 ; > 25% wall involvement Grade 5 ; Whole colonic wall involvement and blood supply injury COLONIC INJURIES
Exteriorized repair Avoided resection Reduced contamination Reduced colostomy Limited in some part of colon Stomal care is more difficult than colostomy COLONIC INJURIES
Primary repair Sutured repair Resection with primary anatomosis COLONIC INJURIES
Primary repair Sutured repair Resection with primary anatomosis COLONIC INJURIES
Primary repair Avoid colostomy Less morbidity than colostomy Gained more popularity Having high risk in patient c underlying medical illness massive blood transfusion COLONIC INJURIES
outcome cause of death exanguination sepsis ; intra- abdominalabscess multi organ failure fistula (primary repair) COLONIC INJURIES
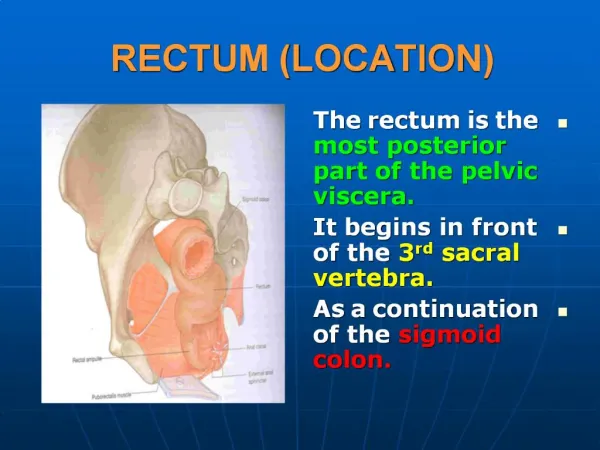
Anatomy Promontary of sacrum to anus intraperitoneal extraperitoneal Length ~12-20 cm. RECTAL INJURIES
Anatomy Anal canal Anorectal ring to anal verge Sphincter complex puborectalis muscle external sphincter internal sphincter RECTAL INJURIES
Etiology Penetrating injuries ; gun shot ~80% Stab & impalement <5% Blunt injury ~ 10% Transanal injury ; ~ 6% Anal intercourse Anal rape Iatrogenic ; enema, thermometer RECTAL INJURIES
Diagnosis Suspected in GSW ; Trunk , buttock , perineum upper thigh Stab ; buttock , perineum , lower abdomen Blood in rectum ( rectal exam ) RECTAL INJURIES
Investigation X-ray pelvis & abdomen; bullet tract,foreign body, fracture pelvis Rigid proctosigmoidoscope Water soluble contrast study RECTAL INJURIES
Treatment 1.Intraperitoneal rectal injuries;as colonic injuriession 2.Extraperitoneal rectal injuries ; Diversion Debridement Distal washout Presacral drainage RECTAL INJURIES
Diversion 1. Loop colostomy 2 .Loop colostomy c stapling distal lumen 3 .End colostomy c mucous fistula 4 .Hartmann’s procedure RECTAL INJURIES
Diversion 1. Loop colostomy 2 .Loop colostomy c stapling distal lumen 3 .End colostomy c mucous fistula 4 .Hartmann’s procedure RECTAL INJURIES
Diversion 1. Loop colostomy 2 .Loop colostomy c stapling distal lumen 3 .End colostomy c mucous fistula 4 .Hartmann’s procedure RECTAL INJURIES
Diversion 1. Loop colostomy 2 .Loop colostomy c stapling distal lumen 3 .End colostomy c mucous fistula 4 .Hartmann’s procedure RECTAL INJURIES
2. Debridement : removed devitalize tissue repair defect if possible severe injury ; resection 3.Distal washout : decrease septic complication RECTAL INJURIES
4.Presacral drainage RECTAL INJURIES
Outcome Cause of death: Sepsis, Multi-organ failure Anorectal abscess Rectal fistula RECTAL INJURIES
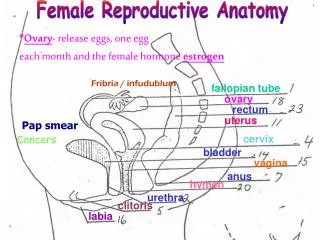
PERINEAL INJURIES • Perineum • Inferior end of trunk • Anterior (urogenital) • Genital organ • Urethra • Posterior (anal) • Anus
PERINEAL INJURIES MALE FEMALE
PERINEAL INJURIES ETIOLOGY : Iatrogenic anorectal injury Traumatic anorectal injury Foreign bodies in rectum Anal intercourse & assult
PERINEAL INJURIES IATROGENIC INJURIES • Obstetric injury • Anorectal surgery • Enema • Rectal thermometer • Urologic & Gynecologic surgery
PERINEAL INJURIES TRAUMATIC INJURIES • Blunt injury • Straddle injury • Laceration • Implement • Gunshot wound • Blast • High pressure
PERINEAL INJURIES MANAGEMENT • Primary survey • Resuscitation • Secondary survey • Definitive care
PERINEAL INJURIES SECONDARY SURVEY • History taking • Cause of injury • Mechanism of injury • Duration of injury • Associated injury • Symptom & sign • Perineal pain • Lower abdominal pain • Bleeding • Sepsis
Perineum , anus , buttock , thigh • Abdomen • Digital rectal examination • Associated injuries • Vagina • Urethra & prostate gland • pelvis PERINEAL INJURIES SECONDARY SURVEY examination
PERINEAL INJURIES INVESTIGATION • Film abdomen supine ,upright , lateral • Rigid sigmoidoscopy • Contrast study
PERINEAL INJURIES TREATMENT • Perineal injury with rectal injury • Debridement • Diversion • Drainage • Distal washout
PERINEAL INJURIES TREATMENT • Perineal injury • Small hematoma ; conservative • Expanded hematoma ; evacuated blood • Laceration ; debridement & stop bleeding • Severe laceration ; debridement , stop bleeding and colostomy
PERINEAL INJURIES TREATMENT • Perineal injury • Debridement • Adequate debridement • Left wound open • Frequent debridement • Adequate pain control • Control contamination
PERINEAL INJURIES TREATMENT • Perineal injury with anal sphincter injury • minimal sphincter injury • severe sphincter injury • colostomy • primary repair • non primary repair
PERINEAL INJURIES TREATMENT • Incontinence • Sphincteroplasty • Muscle transposition • Artificial sphincter
ANAL INTERCOURSE • Mostly in Homosexual • Complication • Retained foreign bodies • Colorectal perforation • Anal tear • Digital rectal exam & sigmoidoscopy
ANAL INTERCOURSE • Management • Uncomplicated injury • Warm sitz bath • Stool softener • Tropical analgesic preparation
ANAL INTERCOURSE • Management • Surgery • Deep tear • Perforation • Sphincter injury • Persistent bleeding
FOREIGN BODIES IN RECTUM • Oral ingested • Bones • Toothpick • Seeds • Anal insertion • Sex toys • Bottles • Cans • Flashlights • Fruit • umbrella
FOREIGN BODIES IN RECTUM • Age ; 20-30 yrs and more than 60 yrs. • Male : female 25: 1 • Classification • Retained F.B. without injury • Non perforative mucosal laceration • Sphincter injury • Rectosigmoid perforation
FOREIGN BODIES IN RECTUM • History • Symptom & sign • Anal or pelvic pain • Inability to remove F.B. • Bleeding • Peritonitis
FOREIGN BODIES IN RECTUM • Physical examination • Abdomen • Digital rectal exam • Investigation • Film abdomen AP& Lateral • Contrast study
FOREIGN BODIES IN RECTUM • Management • Bedside extraction • Local anesthesia • Valsava maneuver • Sedation • Observation