Download
1 / 20
200 likes | 448 Views
#3. Recognize specific syndromes; extra-axial (cerebellopontine, pituitary, frontal) and intra-axial in brain tumor presentation. Extra-axial Tumors. Extrinsic to the brain

E N D
#3. Recognize specific syndromes; extra-axial (cerebellopontine, pituitary, frontal) and intra-axial in brain tumor presentation
Extra-axial Tumors • Extrinsic to the brain • include meningiomas, schwannomas, neurofibromas, and pituitary tumors, craniopharyngiomas as well as mesenchymal tumors of the skull, spine, and dura mater
Meningioma • Derived from arachnoid cap cells of the arachnoid mater • Appear to arise from the dura mater grossly and on MRI: “dural based tumors” • Most common intracranial locations: along the falxcerebri , the convexities and the sphenoid wing. • Less common locations: foramen magnum, olfactory groove, and inside the lateral ventricle
Meningioma • Mostly slow growing, encapsulated, and benign • Malignant may invade adjacent bone or into the cortex • Previous cranial irradiation: risk • Tx: Total resection, post op radiation (atypical and malignant melanoma)
Postcontrast T1-weighted coronal MRI demonstrating a brightly enhancing lesion arising from the falx cerebri with moderate edema and mass effect on the right lateral ventricle. This is a falcine meningioma. Note also the small separate meningioma arising from the dura over the cerebral convexity.
Vestibular Schwannoma (Acoustic Neuroma) • Arise from the superior half of the vestibular portion of the vestibulocochlear nerve (CN VIII) • commonly present with progressive hearing loss, tinnitus, or balance difficulty • Large tumors may cause brain stem compression and obstructive hydrocephalus • Bilateral acoustic neuromas are pathognomonic for neurofibromatosis type 2, a syndrome resulting from chromosome 22 mutation.
Vestibular Schwannoma (Acoustic Neuroma) • Tx: microsurgical resection or with conformal stereotactic radiosurgery (gamma knife or linear accelerator technology) • Complication: damage to the facial nerve (cranial nerve VII)
A. Postcontrast T1-weighted axial MRI demonstrating a brightly enhancing mass on the right vestibular nerve with an enhancing tail going into the internal auditory canal (arrowhead). Pathology demonstrated vestibular schwannoma
Pituitary Adenoma • arise from the anterior pituitary gland (the adenohypophysis). • Microadenoma: <1cm; Macroadenoma >1 cm • Functional (i.e., secrete endocrinologically active compounds at pathologic levels) or nonfunctional (i.e., secrete nothing or inactive compounds). • The most common endocrine syndromes are Cushing's disease due to adrenocorticotropic hormone (ACTH) secretion, Forbes-Albright syndrome due to prolactin secretion, and acromegaly due to growth hormone secretion.
Pituitary Adenoma • Nonfunctional tumors commonly present when larger due to mass effect. • Common symptoms : visual field deficits due to compression of the optic chiasm, or panhypopituitarism due to compression of the gland. • Tx: Surgery (Transphenoidal), medical (Prolactinomas)
Postcontrast T1-weighted sagittal MRI demonstrating a large sellar/suprasellar lesion involving the third ventricle superiorly, and abutting the midbrain and pons posteriorly. The patient presented with progressive visual field and acuity loss. Pathology and lab work revealed a nonfunctioning pituitary adenoma.
Hemangioblastoma • occur almost exclusively in the posterior fossa. • Twenty percent occur in patients with von Hippel-Lindau (VHL) disease, a multisystem neoplastic disorder • Appears as cystic tumors with an enhancing tumor on the cyst wall known as the mural nodule. • Surgical resection is curative for sporadic (non-VHL associated) tumors.
Craniopharyngioma • Benign cystic lesions that occur most frequently in children. • Second peak of occurrence around 50 years of age. • Symptoms result from compression of adjacent structures, especially the optic chiasm, pituitary or hypothalamic dysfunction or hydrocephalus may develop. • Treatment is primarily surgical • Complications: Visual loss, pituitary endocrine hypofunction, diabetes insipidus, and cognitive impairment from basal frontal injury
Neurofibroma • more fusiform and grow within the parent nerve, rather than forming an encapsulated mass off the nerve, as with schwannomas. • They are benign but not encapsulated. • They present similarly to schwannomas and the two may be difficult to differentiate on imaging. • Patients with multiple neurofibromas likely have neurofibromatosis type 1, also known as von Recklinghausen's neurofibromatosis. • Resection for symptomatic lesions should be offered.
Intra-axial Tumors • Intrinsic to the brain
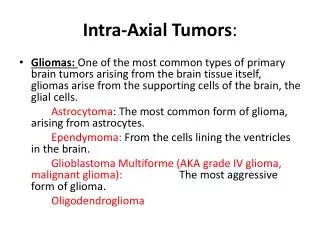
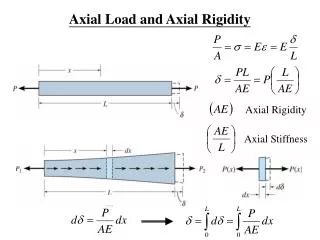
G L I O M A • ASTROCYTOMA: - MOST COMMON PRIMARY INTRA-AXIAL BRAIN TUMOR (low & high grade) - INVOLVE ALL LOBES WITH PREFERENTIAL TO FRONTAL & TEMPORAL LOBES - GRADING BASED ON HISTOLOGY: hypercellularity pleomorphism vascular proliferation necrosis - DIAGNOSIS: CT, MRI, Angiography - TREATMENT: Surgery, Radiation, Chemotheraphy or Combination
OLIGODENDROGLIOMA Treatment: vary from conservative treatment of some patients with serial imaging studies and no intervention to aggressive multimodal treatment including surgical resection, radiotherapy, and chemotherapy
EPENDYMOMA • glial tumors that arise from ependymal cells within the central nervous system (10%)
KEY FEATURES: • USUALLY OCCUR IN THE • FLOOR OF THE 4TH VENTRICLE • POTENTIAL FOR SEEDING THRU • THE NEURAXIS • WORSE PROGNOSIS THE • YOUNGER THE PATIENT; 5 YRS • SURVIVAL AT 80% FOR ADULTS • & 20%-30% IN PEDIATRIC GROUP • MAXIMAL RESECTION FOLLOWED BY • XRT E P E N D Y M O M A