Download
1 / 1
10 likes | 75 Views
DISCUSSION. Mutations. Treatment naïve: % of patients with 1 primary mutation by calendar year. Frequently observed mutations. Recent infection. Temporal and demographic patterns. Prevalence of resistance by demographic factors. METHODS. RESULTS. BACKGROUND. NRTI. NNRTI. PI.

E N D
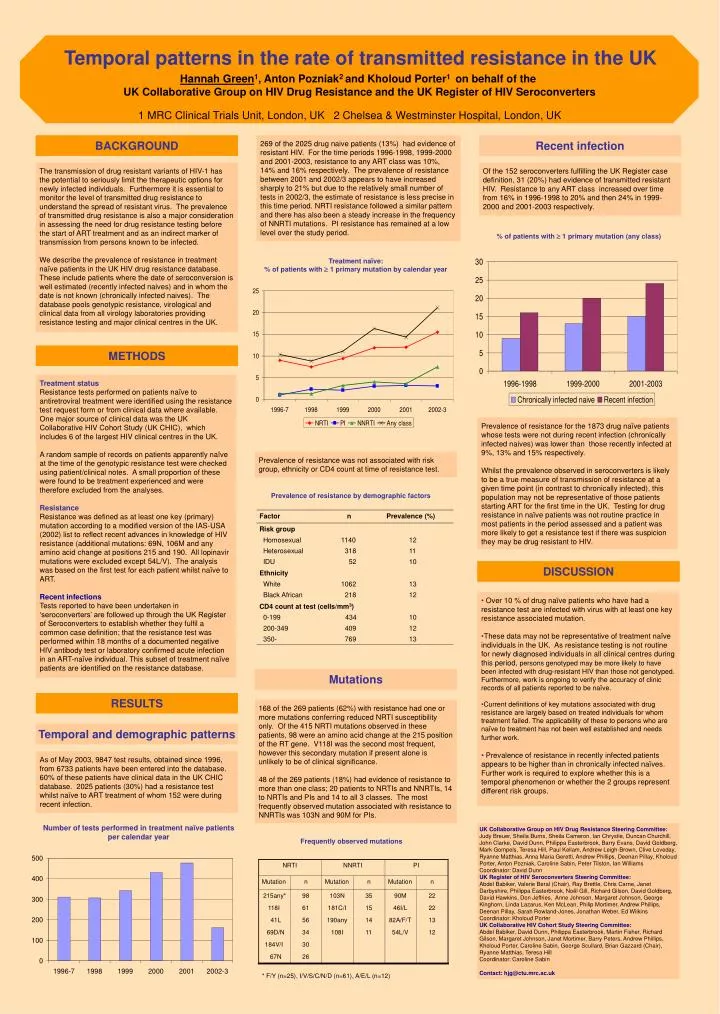
DISCUSSION Mutations Treatment naïve:% of patients with 1 primary mutation by calendar year Frequently observed mutations Recent infection Temporal and demographic patterns Prevalence of resistance by demographic factors METHODS RESULTS BACKGROUND NRTI NNRTI PI Mutation n Mutation n Mutation n 215any* 98 103N 35 90M 22 118I 61 181C/I 15 46I/L 22 41L 56 190any 14 82A/F/T 13 69D/N 34 108I 11 54L/V 12 184V/I 30 67N 26 * F/Y (n=25), I/V/S/C/N/D (n=61), A/E/L (n=12) Factor n Prevalence (%) Risk group Homosexual 1140 12 Heterosexual 318 11 IDU 52 10 Ethnicity White 1062 13 Black African 218 12 CD4 count at test (cells/mm3) 0-199 434 10 200-349 409 12 350- 769 13 Temporal patterns in the rate of transmitted resistance in the UK Hannah Green1, Anton Pozniak2 and Kholoud Porter1 on behalf of the UK Collaborative Group on HIV Drug Resistance and the UK Register of HIV Seroconverters 1 MRC Clinical Trials Unit, London, UK 2 Chelsea & Westminster Hospital, London, UK 269 of the 2025 drug naive patients (13%) had evidence of resistant HIV. For the time periods 1996-1998, 1999-2000 and 2001-2003, resistance to any ART class was 10%, 14% and 16% respectively. The prevalence of resistance between 2001 and 2002/3 appears to have increased sharply to 21% but due to the relatively small number of tests in 2002/3, the estimate of resistance is less precise in this time period. NRTI resistance followed a similar pattern and there has also been a steady increase in the frequency of NNRTI mutations. PI resistance has remained at a low level over the study period. The transmission of drug resistant variants of HIV-1 has the potential to seriously limit the therapeutic options for newly infected individuals. Furthermore it is essential to monitor the level of transmitted drug resistance to understand the spread of resistant virus. The prevalence of transmitted drug resistance is also a major consideration in assessing the need for drug resistance testing before the start of ART treatment and as an indirect marker of transmission from persons known to be infected. We describe the prevalence of resistance in treatment naïve patients in the UK HIV drug resistance database. These include patients where the date of seroconversion is well estimated (recently infected naives) and in whom the date is not known (chronically infected naives). The database pools genotypic resistance, virological and clinical data from all virology laboratories providing resistance testing and major clinical centres in the UK. Of the 152 seroconverters fulfilling the UK Register case definition, 31 (20%) had evidence of transmitted resistant HIV. Resistance to any ART class increased over time from 16% in 1996-1998 to 20% and then 24% in 1999-2000 and 2001-2003 respectively. % of patients with 1 primary mutation (any class) Treatment status Resistance tests performed on patients naïve to antiretroviral treatment were identified using the resistance test request form or from clinical data where available. One major source of clinical data was the UK Collaborative HIV Cohort Study (UK CHIC), which includes 6 of the largest HIV clinical centres in the UK. A random sample of records on patients apparently naïve at the time of the genotypic resistance test were checked using patient/clinical notes. A small proportion of these were found to be treatment experienced and were therefore excluded from the analyses. Resistance Resistance was defined as at least one key (primary) mutation according to a modified version of the IAS-USA (2002) list to reflect recent advances in knowledge of HIV resistance (additional mutations: 69N, 106M and any amino acid change at positions 215 and 190. All lopinavir mutations were excluded except 54L/V). The analysis was based on the first test for each patient whilst naïve to ART. Recent infections Tests reported to have been undertaken in ‘seroconverters’ are followed up through the UK Register of Seroconverters to establish whether they fulfil a common case definition; that the resistance test was performed within 18 months of a documented negative HIV antibody test or laboratory confirmed acute infection in an ART-naïve individual. This subset of treatment naïve patients are identified on the resistance database. Prevalence of resistance for the 1873 drug naïve patients whose tests were not during recent infection (chronically infected naives) was lower than those recently infected at 9%, 13% and 15% respectively. Whilst the prevalence observed in seroconverters is likely to be a true measure of transmission of resistance at a given time point (in contrast to chronically infected), this population may not be representative of those patients starting ART for the first time in the UK. Testing for drug resistance in naïve patients was not routine practice in most patients in the period assessed and a patient was more likely to get a resistance test if there was suspicion they may be drug resistant to HIV. Prevalence of resistance was not associated with risk group, ethnicity or CD4 count at time of resistance test. • Over 10 % of drug naïve patients who have had a resistance test are infected with virus with at least one key resistance associated mutation. • These data may not be representative of treatment naïve individuals in the UK. As resistance testing is not routine for newly diagnosed individuals in all clinical centres during this period, persons genotyped may be more likely to have been infected with drug-resistant HIV than those not genotyped. Furthermore, work is ongoing to verify the accuracy of clinic records of all patients reported to be naïve. • Current definitions of key mutations associated with drug resistance are largely based on treated individuals for whom treatment failed. The applicability of these to persons who are naïve to treatment has not been well established and needs further work. • Prevalence of resistance in recently infected patients appears to be higher than in chronically infected naïves. Further work is required to explore whether this is a temporal phenomenon or whether the 2 groups represent different risk groups. 168 of the 269 patients (62%) with resistance had one or more mutations conferring reduced NRTI susceptibility only. Of the 415 NRTI mutations observed in these patients, 98 were an amino acid change at the 215 position of the RT gene. V118I was the second most frequent, however this secondary mutation if present alone is unlikely to be of clinical significance. 48 of the 269 patients (18%) had evidence of resistance to more than one class; 20 patients to NRTIs and NNRTIs, 14 to NRTIs and PIs and 14 to all 3 classes. The most frequently observed mutation associated with resistance to NNRTIs was 103N and 90M for PIs. As of May 2003, 9847 test results, obtained since 1996, from 6733 patients have been entered into the database. 60% of these patients have clinical data in the UK CHIC database. 2025 patients (30%) had a resistance test whilst naïve to ART treatment of whom 152 were during recent infection. Number of tests performed in treatment naïve patients per calendar year UK Collaborative Group on HIV Drug Resistance Steering Committee: Judy Breuer, Sheila Burns, Sheila Cameron, Ian Chrystie, Duncan Churchill, John Clarke, David Dunn, Philippa Easterbrook, Barry Evans, David Goldberg, Mark Gompels, Teresa Hill, Paul Kellam, Andrew Leigh-Brown, Clive Loveday, Ryanne Matthias, Anna Maria Geretti, Andrew Phillips, Deenan Pillay, Kholoud Porter, Anton Pozniak, Caroline Sabin, Peter Tilston, Ian Williams Coordinator: David Dunn UK Register of HIV Seroconverters Steering Committee: Abdel Babiker, Valerie Beral (Chair), Ray Brettle, Chris Carne, Janet Darbyshire, Philippa Easterbrook, Noël Gill, Richard Gilson, David Goldberg, David Hawkins, Don Jeffries, Anne Johnson, Margaret Johnson, George Kinghorn, Linda Lazarus, Ken McLean, Philip Mortimer, Andrew Phillips, Deenan Pillay, Sarah Rowland-Jones, Jonathan Weber, Ed Wilkins Coordinator: Kholoud Porter UK Collaborative HIV Cohort Study Steering Committee: Abdel Babiker, David Dunn, Philippa Easterbrook, Martin Fisher, Richard Gilson, Margaret Johnson, Janet Mortimer, Barry Peters, Andrew Phillips, Kholoud Porter, Caroline Sabin, George Scullard, Brian Gazzard (Chair), Ryanne Matthias, Teresa Hill Coordinator: Caroline Sabin Contact: hjg@ctu.mrc.ac.uk