Download
1 / 50
510 likes | 667 Views
Explore pelvic anatomy, joints, planes, and sizes for clinical evaluation. Learn about different pelvic shapes and estimation methods.

E N D
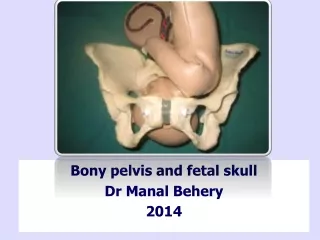
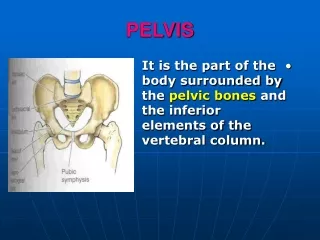
THE BONY PELVIS a. Pelvic anatomy b. Pelvic joints c. Planes & diameters of the pelvis d. Pelvic shapes e. Pelvic size and its clinical estimation
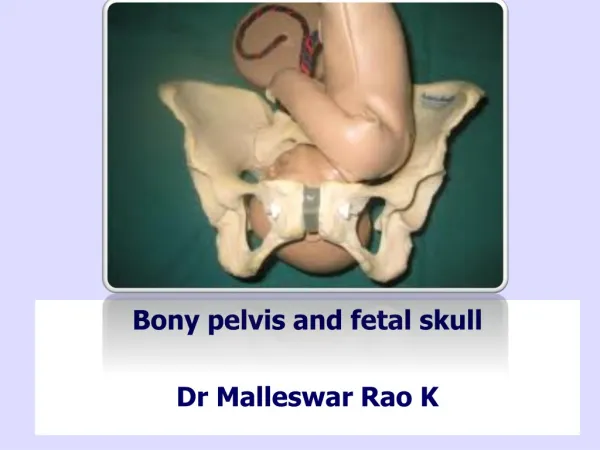
a. PELVIC ANATOMY b. PELVIC JOINTS - Symphysis pubis - Sacroiliac joints - Relaxation of the pelvic joints ( especially during pregnancy)
PLANES AND DIAMETER OF THE PELVIS HAVING 4 IMAGINARY PLANES : 1. The plane of the pelvic inlet ( Superior strait ) 2. The plane of the pelvic outlet ( Inferior strait ) 3. The plane of the mid pelvis ( least pelvic dimensions ) 4. The plane of greatest pelvic dimensions ( Has no obstetrical significance , it is not considered further)
HODGE PLANE I = Pelvic inlet II Hodge I through lower margin of the symphysis III Hodge I through ischial spine IV Hodge I through the tip of coccygis
PELVIC SHAPES CALDWELL - MOLOY CLASSIFICATION (1933 - 34) Gynecoid pelvis Android pelvis Anthropoid pelvis Platypelloid pelvis
GYNECOID PELVIS - Almost 50% of white women (Todd’ Collection study) - Ascertained the frequency of the four parent pelvic types by study of Todd’s Collection ( Caldwell & CoWorkers,1939) ANDROID PELVIS - 1/3 of pure type pelvis ( white women), 1/6 non white women - The extreme android pelvis presages poor prognosis for vaginal delivery - The frequency of difficult forceps operations increases
ANTHROPOID PELVIS - 1/4 pure type pelvis in white women and nearly 1 1/2 of those in non white women PLATYPELLOID PELVIS - Rarest of the pure varieties ( < 3% ) INTERMEDIATE TYPE PELVIS - Mixed type - More frequent than pure types
PELVIC SIZE AND ITS CLINICAL ESTIMATION - Pelvic inlet measurements - Diagonal conjugate - Engagerment : - with engagerment, the fetal head serves as an internal pelvimeter to demonstrate that the pelvic inlet is ample for that fetus.
PELVIC INLET - Obstetrical conjugate ( normal > 10 cm) - Diagonal conjugate CD - 1.5 to 2 cm = True conjugate
PELVIC OUTLET MEASUREMENTS ( diameter between the ischial tuberosities ) Called as : - Biischial diameter , Inter tuberous diameter, Transverse diameter of the outlet - The shape of the sub pubic arch also can be evaluated at the same time by palpating the pubic rami from the sub pubic region toward the ischial tuberosities. - Estimated by placing a closed fist against the perineum between the ischial tuberosities, after fist measuring the width of the closed fist ( usually > 8 cm )
MID PELVIS ESTIMATION - Clinical estimation of mid pelvis capacity by any direct form of measurement is not possible - Suspicion contracted pelvis in this region : - Ischial spines are quite prominent - The side walls are felt to converge - The concavity of the sacrum is very shallow - Ischial diameter of the outlet < 8 cm
Outer measurement • Distantia spinarum • Distantia cristarum • External conjugate (Baudelaque) • Vaginal examination
95 % of all labors is in vertex presentation and most commonly ascertained by abdominal palpation and confirmed by vaginal examination • Majority of cases the vertex enters the pelvis with the sagittal suture in the transverse pelvic diameter • The fetus enters the pelvis in the Left Occiput Transverse Position / LOT (40% of labors) & 20% ROT. • The head either enters the pelvis with the occiput rotated 45o anteriorly from the transverse position
20 % of all labors the fetus enters the pelvis in an Occiput Posterior (OP) position. • The ROP is slightly more common than LOP and posterior positions are more often associated with a narrow forepelvis • The head either enters the pelvis with the occiput rotated 45o anteriorly from the transverse position
THE CARDINAL MOVEMENTS OF LABOR ARE : • ENGAGEMENT • DESCENT • FLEXION • INTERNAL ROTATION • EXTENSION • EXTERNAL ROTATION • EXPULSION
ENGAGEMENT • The biparietal diameter, the greatest transverse diameter of the fetal head in occiput presentations, passes through the pelvic inlet is designated engagement (during the last few weeks of pregnancy) • A normal – sized head usually does not engage with its sagittal suture directed anteroposteriorly. • Instead, the fetal head usually enters the pelvic inlet either in the transverse diameter or in one of the oblique diameters.
ASYNCLITISM • Although the fetal heads tends to accommodate to the transverse axis of the pelvic inlet, the sagittal suture , while remaining parallel to that axis, may not lie exactly midway between the symphysis and sacral promontory • The sagittal suture frequently is deflected either posteriorly toward the promontory or anteriorly toward the symphysis. • Such lateral deflection of the head to a more anterior or posterior position in the pelvis is called asynclitism • Moderate degrees of asynclitism are the rule in normal labor, but if severe , may lead to CPD
DESCENT • In nulliparas, engagement may take place before the onset of labor and further descent may not follow until the onset of second stage. In multiparous women, descent usually begins with engagement. • Descent is brought about by one or more of four forces : • Pressure of the amniotic fluid • Direct pressure of the fundus upon the breech with • contractions • Bearing down efforts with the abdominal muscles • Extensions and straightening of the fetal body