Download
1 / 11
110 likes | 301 Views
Definition. Inflammation of the middle ear nearly always preceded by an URTI. . Causes. Organisms in children include viruses (min. 25%), Haemophilus influenzae (25%), Moraxella catarrhalis(15%), Streptococcus pneumoniae (25%) and Staphlococcus aureus (2%). Organisms in adults include viruses most

E N D
1. Otitis Media Lawrence Pike
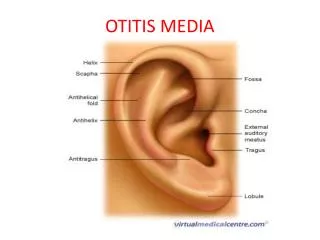
2. Definition Inflammation of the middle ear nearly always preceded by an URTI.
3. Causes Organisms in children include viruses (min. 25%), Haemophilus influenzae (25%), Moraxella catarrhalis(15%), Streptococcus pneumoniae (25%) and Staphlococcus aureus (2%).
Organisms in adults include viruses most commonly.
The term recurrent is defined as 3 or more episodes in 6 months, or 4 or more in a year.
4. Incidence Approximately 40% of children suffer one or more episodes before the age of 10 years. More cases are seen in the winter months.
Uncommon in adults.
5. Symptoms Pain
Usual onset at night and severe for 12 hrs, then settles and niggles for 3-5 days
Discharge can occur (and often relieves pain)
Fever, vomiting and loss of appetite may occur, especially in young children.
Occasionally tinnitus, voice resonance, giddiness and sickness occur.
Irritability may be the only indication in infants.
Hearing loss occurs if accumulation of fluid has taken place.
6. Signs change of colour of the tympanic membrane to pink/red
bulging drum
loss of outline of drum and landmarks
discharge in meatus
perforation.
there may be tenderness over the mastoid.
7. Risk Factors Passive smoker
Male
Family history of otitis media.
In day care
On formula feed
8. Differential Diagnosis Furuncle or diffuse otitis externa
Post auricular adenitis
Referred otalgia (eg from teeth)
Herpetic lesion of ear
9. What can go wrong? Progression to glue ear or perforation. Rarely to mastoiditis, labyrinthitis, meningitis, intracranial sepsis or facial nerve palsy.
Recurrent episodes may lead to atrophy and scarring of the eardrum, chronic perforation and otorrhoea, cholesteatoma, permanent hearing loss, chronic mastoiditis and intracranial sepsis.
10. Treatment 80% will resolve within 3 days without treatment, 95% in 5 days
Antibiotics may improve short term symptoms, although evidence for any gain in medium to long term outcome is lacking
Countries with lower rates of antibiotic prescribing for acute otitis media do not have an increase in the number of complications
The Standing Medical Advisory Committee concluded that 'antibiotics are probably unnecessary in acute otitis media. Reassurance, time and adequate pain relief are required.'
11. Treatment Simple analgesia
Paracetamol
Ibuprofen (some evidence superior)
There are no published controlled trials to support the use of antihistamine and decongestant preparations.
12. Antibiotic Treatment (if chosen) Children and Adults
Amoxycillin limited to three days [SMAC 1998]
In patients with penicillin allergy
Clarithromycin or azithromycin are both effective and are active against the common pathogen H influenzae.
Erythromycin may be useful, although it lacks activity against H. influenzae