Download
1 / 50
560 likes | 975 Views
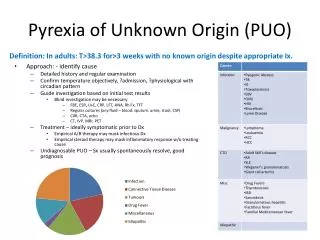
Pyrexia of Unknown Origin. Stephen Hughes MRCPCH PhD Consultant Paediatric Immunologist. PRE-TEST. The commonest cause of PUO is: A common disease presenting in an atypical way. A rare disease presenting in atypical way. A common disease presenting typically.

E N D
Pyrexia of Unknown Origin Stephen Hughes MRCPCH PhD Consultant Paediatric Immunologist
PRE-TEST • The commonest cause of PUO is: • A common disease presenting in an atypical way. • A rare disease presenting in atypical way. • A common disease presenting typically. • A rare disease presenting typically.
The answer is ..A • ..The commonest cause of PUO IS • …Common disease presenting • ATYPICALLY
What is a PUO? Reid Petersdorf & Beeson Dechovitz & Moffet
Malignancies • Are much more common in adults • (40 vs. 10%). • Either because of infection or cytokines • Most commonly: • Lymphoma • Leukaemia • Neuroblastoma • Sarcomas and Hepatomas } 80% of malignancies with PUO
Who should have a BMA? • Patients with suggestive blood film / count or other evidence pointing to Leukaemia / Lymphoma • Culture for TB, Salmonella, Leishmania
Infection frequencies • Infectious mononucleosis (EBV or CMV) (up to 20%) • Other viruses (NB. measles, hepatitis, HIV (up to 15%) • UTI (up to 15%) • Pneumonia (up to 10%) • Various URTIs (up to 10%) • Endocarditis (Staph. Strep. HACEK, Bruce, Cox, Rick) (up to 5%) • Tuberculosis (up to 5%) • Streptococcosis (up to 5%) • Bartonella (cat scratch disease) (up to 5%) • Meningitis / para meningeal abscess (up to 5%) • Enteric infection (Salmonella, Yersinia) (up to 5%) • Malaria (up to 1%) • Brucella (up to 1%) • HSV (generalised but occult) (up to 1%)
Infectious mononucleosis • Diagnosis is made by EBV PCR on blood (EDTA) • Support is offered by • Atypical lymphocytes (a late finding, in some) • Heterophile antibodies (IgM binding sRBCs) • IgM antibodies to EBV • Other causes include • CMV, Toxoplasma, HIV, Rubella, HepAB, HHV678
Endocarditis • If the child has congenital or acquired cardiac disease, endocarditis must be excluded. • If there is no pre-morbid cardiac disease, is endocarditis possible? Y • In which patients: those with lines • What chance of endocarditis if there are no risk factors and no signs? <5% • What are the critical tests? BC, BC, BC
How do I get the ECHO? • Is there a risk factor? • Is there a new murmur? • Is there a BC positive for Staph or viridans Strep? • 5-10% of IE have negative BCs • Because of antibiotics or • Fastidious organisms (HACEK) or • Aspergillus, Bart, Bruce, Cox, Rick, Mycobacteria, Noca, Chlamydia, viruses…
How do I get the ECHO? • Is there splenomegaly, emboli, petechiae, splinters, clubbing, Osler nodes, Roth spots, Janeway lesions or haematuria • What is the ESR and the RF? • Remember, the sensitivity of TTE is 80%. TOE can be considered if the Duke criteria require it later in the period of assessment
Bart, Bruce, Rick & Cox • Bartonella (5) - the cat scratch illness, usually regional adenopathy, sometimes PUO. Sometimes HSM, sometimes Haem abnormalities. Diagnosis by serology. • Brucella (1) - must have exposure (farm animal contact or unpasteurised milk). LFTs rise. Diagnosis by serology. • Rickettsia (0) - imported. • Coxiella (0) - Q fever, cats and unpasteurised milk. Diagnosis by serology.
Could it be TB? • Yes
History • Full history and examination (repeatedly) • Travel • Pets • Contact with ticks • Contact with animals • Drinking unpasteurised milk • Cardiac disease • Dental history • Growth • Drugs
Investigations (step 1) • Decision to investigate fever (arrival): verify fever • Urinalysis and culture unless it is on the list, • Blood culture it won’t get done • Throat swab • FBC (and film) • CRP (and ESR) (if the blood flows, take it) • NPS for viruses Could it be ‘flu? • Stool culture with OCP if travelled Salmonella? • For consideration at 5 days - is this Kawasaki? • If it is, store serum now
Investigations (step 2) • By days 5-7, if any focal signs or symptoms appeared, follow them. • Carefully record antimicrobial prescriptions • Do anything missed from step 1 and organise: • CXR occult pneumonia • LP occult meningitis • More BC yield rises • ASOT Streptococcosis is common • Coagulation abnormalities will direct inv • Ferritin massive elevation helpful • Serum to be saved acute serology • Request BMA If haem abnormal • US Abdomen harmless / helpful
Investigations (step 3) • By days 10-14, if no diagnosis is reached and not already done: • ANA, dsDNA, C3, C4, ENA, Cardiolipin, RF 20% risk • Lupus anticoagulant (if clotting abnormal) • ECG, ECHO, converse with cardiology 1-5% risk • Mantoux, QFG, ESR, Gastric lavage / sputum 1-5% risk • LP (if not already done) 1-5% risk • CT of any suspect region • Brain, Chest, Abdo, ENT • Bone scan for pelvic, skeletal osteomyelitis • Serology for Bartonella 5% risk • Serology for HIV, other microbes and save serum
Investigations (step 4) • By day 21, • Review everything again… • TFTs • CT abdomen (regardless of signs) • Biopsy of abnormal tissue, inc: • LNs • Gut • Skin • (Liver) • Define immune status of child (call the immunologist) • Stop drugs, if started • Wait for clues.
Endocrine causes for PUO • Hyperthyroidism • Occasionally cause PUO → most frequently diagnosed clinically. • Often accompanied by weight loss. • No local neck pain and typically enlarged non-tender thyroid. • Adrenal • Rare, potentially fatal, but eminently treatable cause of PUO. • Consider if: nausea/vomit, ↓weight, ↓BP, ↓Na & ↑K.
Rheumatology and PUO • 10-20% of cases in most series • In the earlier series, Rheumatic fever was key • More recently, SoJIA > SLE > vasculitis (PAN, Behcet, WG) & HLH > Sarcoidosis
A case • 14 year old girl with one month history of fever and malaise … • She received 10 days amoxicillin from GP but no response … • On exam, T = 38.4°C … several lymph nodes in the neck … non-tender and rubbery …
You want a what? PubMed Google Consultation CXR Tea Biopsy US Abdomen Blood culture ECHO CT Other Tests Bloods ASOT TB tests PCRs Throat swab BMA HIV test Urinalysis
Serology • Complement fixation tests for Mycoplasma, Chlamydia, Adenovirus, Legionella, Coxiella were all available. Convalescent specimens are awaited. • Samples were sent for Toxoplasma, Bartonella, Brucella, EBV, CMV… • We have a brief (two week) wait…
ASOT • ASOT is negative.
Biopsy • Seriously, no. • Sorry, not today. • There are 5 children about to breach their 20 week wait for routine surgery. • Your request is noted and will be processed through the usual channels, but please don’t hesitate to make another choice.
Tests of immunity • What on earth are we looking for? Q. is she immune suppressed? Q. What is the diagnosis? Q. Evidence for recent immune dysregulation (Igs, B and T cells)
Immune Function • History tells you about immune suppression. • Immune function is harder. • T cell numbers are normal. • There are no abnormalities on routine testing
What is the diagnosis? • Tests of immunity aren’t going to help you. • The serologies are all negative.
Immune Dysregulation • She does make immunoglobulin: lots of it - • IgG 18.2, IgA 1.2, IgM 4.8 • She has all the right cells.
Consultation • Good idea. • With whom shall we consult? • Respiratory, ENT, Endocrinology, Bone, Rheumatology, Infection, Immunology, Gastroenterology, Haematology, Cardiology, Intensive care?
Abdominal ultrasound • Normal
Blood cultures • Negative at 5 days
Urinalysis • Normal urine on dipstick, no cells on microscopy and no growth
Hb 13.2 MCV 95 Plt 252 WBC 3.2 N 1.8 L 1.0 M 0.3 E 0.1 ESR 42 U&E normal Alb 32 ALT 50 LDH 378 CRP 24 Haem & Biochemistry
PCRs • EBV, CMV, HHV6, HHV7, HHV8 are negative • Adeno is negative • Hep A and B are negative
Additional tests Immunology Serology
HIV test • Negative
TB tests • Mantoux negative • Quantiferon Gold negative • No contact history • No AAFB seen on any sample. • Cultures still awaited many weeks later.
Bone marrow aspirate • Haematologists will do it, but reluctantly. • Suggests you arrange imaging and then a biopsy of a node
Tea • You cannot have tea until you are finished the exercise.
ECHO • Normal structure. • Normal flows. • No shunts or leaks. • Satisfactory function. • Pressures could not be determined because of anatomical integrity.
Biopsy Necrotising histiocytic lymphadenitis Absent neutrophils Normal histiocytes and lymphocytes
Diagnosis made • Kikuchi Fujimoto syndrome • A disease most commonly of young Asian women. • Usually lymphadenitis of cervical chain • Can cause PUO • Mimics TB / lymphoma • Diagnosis made by pathologist
Thanks for participating • Assessment of a fever is dominated by history and examination • Repeated assessment probably has more value than blind screening • Uncommon presentation of common illness is the norm • Involvement of colleagues is critical • With longer fever the cause is either more benign or more malign