Download
1 / 39
400 likes | 556 Views
Acute Hypoxemic Respiratory Failure. Margaret J. Neff, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care. “Your patient’s sat is 88%”. 55 y/o man with a history of mild COPD 3 days s/p elective surgery bilateral knee replacements

E N D
Acute Hypoxemic Respiratory Failure Margaret J. Neff, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care
“Your patient’s sat is 88%” • 55 y/o man with a history of mild COPD • 3 days s/p elective surgery • bilateral knee replacements • Uneventful post-operative course except for an ileus and ongoing complaints of pain • Had been on room air during the day • You’re called with this sat at 3 a.m.
“He says he can’t catch his breath” • Repeat sat confirmed: 88% • CXR done in the a.m. had shown mild bibasilar atelectasis • possible RLL infiltrate • ABG: 7.45/32/60 on room air • On high flow oxygen, his PaO2 is 100
Causes of Hypoxemia • Decreased PiO2 • Hypoventilation • Diffusion abnormality • Ventilation/Perfusion mismatch • Dead space (high V/Q) • Shunt (low V/Q)
Decreased PiO2 • High altitude • Iatrogenic • i.e. wrong gas mixture • Unlikely to be an issue in clinical hypoxemia • Aa gradient normal
Hypoventilation • Essentially alveolar hypoventilation • CNS drive depressed • Pain and splinting • Thoracic or abdominal restriction • Commonly seen clinically • May be manifest as bibasilar atelectasis • Hypoxemia reverses if take deep breath • Aa gradient normal
Diffusion Abnormality • Acute or chronic disease which affects the ability for oxygen to transport from alveolus to capillary • Common in moderate to severe lung disease, vascular disease, etc • Unlikely to cause acute hypoxemia • Aa gradient increased
Ventilation/Perfusion MismatchDead Space • Areas with normal ventilation, reduced perfusion (high V/Q ratio) • Pulmonary embolus is a good example • Dead space and poor CO2 removal require increased minute ventilation • May or may not be hypoxemia • Aa gradient increased
Ventilation/Perfusion MismatchShunt • Areas with decreased ventilation and normal perfusion (low V/Q) • Consolidation from pneumonia • Can increase if lose ability for hypoxic pulmonary vasoconstriction • non-selective vasodilators: nitrates, nipride • Poorly oxygen responsive • Aa gradient increased
“Your patient is still SOB” • Unlikely a problem with PiO2 or diffusion • May be some degree of hypoventilation due to narcotic use • Sputum with lots of polys and GPC • Repeat CXR shows consolidated RLL • Other possibilities?
“Your next admit is here” • 45 y/o man with diabetes and urosepsis • progressively hypotensive, tachypneic • Intubated for respiratory distress and hypoxemia: oxygen sat on high flow oxygen of 90%
Effusion or Edema? • “Bilateral infiltrates consistent with pulmonary edema” • meets radiographic criteria for acute lung injury CT reveals normal parenchyma but bilateral effusions Courtesy of G. Rubenfeld
Pleural Effusion 1 day later After CT insertion
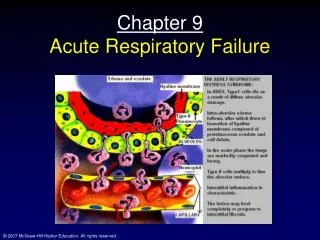
Acute Lung Injury (ALI) • Clinical diagnosis (AECC definition) • CXR: bilateral infiltrates consistent with pulmonary edema • PaO2/FiO2 ratio < 300 (< 200 for ARDS) • No evidence of left atrial hypertension • PAWP < 18 if available AJRCCM 1994
ALI Risk Factors • Trauma • Sepsis • Aspiration • Multiple transfusions • Pancreatitis, overdose, near drowning • Still up to 20% of patients without a defined risk factor • in other words, don’t have to have a risk to have ALI/ARDS
ALI Pathophysiology • Inflammatory process and increased vascular permeability • Bronchoalveolar lavage fluid: neutrophil predominant • those with persistent neutrophils in BAL tend to have a worse clinical course
ALI: clinical manifestations • Early in the course of ARDS, hypoxemia often dominant • Due primarily to intrapulmonary shunting • atelectasis and alveolar flooding • disruption of normally protective hypoxic pulmonary vasoconstriction
ALI: clinical manifestations • After 3-7 days, poor compliance can become the major problem • fibroproliferative stage • Increasing dead space (can exceed 70%) • fibrosis, microthrombi in vessels • can lead to pulmonary hypertension and right heart dysfunction
ALI: Management • Lung protective ventilation • 22% reduction in mortality • Tidal volume 6 ml/kg (PBW) • Pst < 30 cmH2O • allowing pH down to 7.15 if necessary • confirms previous animal studies showing increased systemic inflammation with higher tidal volumes, precipitated by lung stretch NEJM 2000
Other Potential Therapies • Prone positioning? • Steroids? • Anti-inflammatory agents? • Surfactant? • Anti-oxidants? • Inhaled nitric oxide? NONE PROVEN
Corticosteroids • Hypothesized to be effective due to intense inflammatory response seen in ARDS patients • Bronchoalveolar lavage with >70% neutrophils (normally < 2%) • Plasma IL6 levels elevated • Previous studies using steroids early in ARDS have not proven beneficial1 1 Crit Care Med 23:1294-1303
Steroids Late in ARDS • After first 3-7 days, ARDS progresses in many patients to a fibrotic stage • Proliferation of alveolar type II cells • Several small studies of steroids at this phase1 • Inconclusive, in part due to study design • Possibly due to the need for a balance of pro- and anti-inflammatory mediators 1 JAMA 280:159-165
Recent Steroid Trial • NIH sponsored ARDS network (“LaSRS”) • 10 sites nationally conducting ARDS studies • Enrolled patients at day 7-28 of ARDS • Receive steroids 2mg/kg/d (tapered over 2 weeks) • 180 patients enrolled • No difference in mortality (increased with steroids if given >14 days after ALI) • Steroids: more vent-free days, shock-free days; also more neuromuscular complications NEJM 2006; 354(16):1671
FACTT Study • Liberal vs conservative fluid mgmt • No difference in mortality • Conservative strategy resulted in better lung fxn and shorter time on vent & in ICU • Fluid strategy initiated after shock resuscitation • PAC vs CVC • No difference in mortality • More complications in PAC NEJM 2006; 354(21):2213-24 & NEJM 2006;354(24):2564-75
What else can we do for ARDS patients? • Minimize ICU-related complications • HOB elevation • DVT prophylaxis • Stress gastritis prophylaxis • Optimizing nutrition • Early enteral feeding +/- TPN • Invasive diagnostic strategies for ventilator-associated pneumonia • Tight glucose control • Sedation management
RCT of HOB Elevation • 1 year enrollment in MICU (Spain) • Randomized to HOB > 45° or supine • Excluded if recent abd or neurosurgery, refractory shock, re-intubation • Endpoint: clinically or microbiologically confirmed pneumonia • (not rigorously defined, though) • 86 patients enrolled • Mean age 65yr; 34% with COPD Lancet 1999;354:1851-8
Results • Nosocomial pneumonia lower in semi-recumbent group • 8% vs 34% for clinically suspected • 5% vs 23% for micro proven • Supine position and enteral feeding were independent risk factors for VAP • Highest risk when both occurred together
Ventilator Associated Pneumonia • Often difficult diagnosis to make clinically • CXR in ALI patient is already abnormal • ET aspirates may just reflect colonization • May be on antibiotics for surgical procedures or other infections
VAP Diagnosis • RCT of 413 patients intubated for at least 48 hours1 • Clinical suspicion of VAP • No antibiotic change for prior 72 hours • Bronchoscopy vs ET aspirate • Bronch: Reduced mortality at day 14, decreased antibiotic use, more antibiotic free days, more appropriate abx choices 1 Ann Intern Med 2000;132:621-30
Tight Glucose Control In ICU • Recognized hyperglycemia/insulin resistance in ICU patients • RCT of glucose control in SICU patients • 2/3 cardiac surgery patients • 13% with h/o diabetes • Glucose goals: 80-110 vs 180-200 • Decreased mortality • (ICU) 4.6% vs 8%; (hospital) 10.9% vs 7.2% • Subsequent studies show benefit > 4yrs for CV surg patients; questions results in MICU N Engl J Med 2001;3451359-67; Eur Heart J 2006 Apr 11 Epub; NEJM 2006 354(5):449-61
Interruption of Sedative Infusions in the ICU • Prospective, randomized trial • 150 patients receiving continuous infusions • Targeted Ramsay 3-4 • Randomized to daily interruption of infusion or standard care • The intervention was disruption of infusion, not controlling dosing or sedation targets • Once patient awake, investigator notified primary team and decision made regarding resuming infusion (not based on protocol) Kress, et al. NEJM 2000; 342:1471-7
Better Outcomes with Interruption of Sedative (& Analgesic) Infusion • 2 fewer days on ventilator (5 days vs 7) • 3.5 fewer days in the ICU (6.5 vs 10) • Fewer diagnostic tests to work up altered mental status (9% vs 27%) • No difference in complications • e.g. self-extubations (4% vs 7%)
Does Deep Sedation Predispose to PTSD? • Factual memory protected against post-traumatic stress disorder symptoms • Delusional memory was a risk for PTSD • Implications: • Deep sedation and complete amnesia may not be beneficial to patients • Side effects of drugs (hallucinations, nightmares) may be harmful Jones, et al. Crit Care Med 2001;29:573-80
ALI: Outcomes • Improved mortality over the past 30 years • 60% mortality reduced to 30-40% • Most continue to improve lung function over the first year • often left with abnormal diffusion capacity • Evidence to suggest some loss in neuropsychiatric function/testing and neuromuscular function
Respiratory Failure • Your 2 patients did well • Patient with pneumonia continued to improve and transferred to rehab • Patient with urosepsis was in the ICU for 7 days with ALI but was extubated and doing well.
Acute Respiratory Failure • When faced with acute SOB, run through the list of possibilities while initiating diagnostic testing and applying oxygen • Think of the clinical scenario to help you trim the possibilities • See if interventions help • Diagnose and treat for the most life-threatening while you’re fine-tuning the diagnosis