Download
1 / 17
190 likes | 781 Views
Cerebral Malaria. severe complication of falciparum malaria mortality of 30-50% associated with sequestration in micro-vasculature of brain a diffuse encephalopathy with loss of consciousness consciousness ranges from stupor to coma unresponsive to pain, visual, and verbal stimuli

E N D
Cerebral Malaria • severe complication of falciparum malaria • mortality of 30-50% • associated with sequestration in micro-vasculature of brain • a diffuse encephalopathy with loss of consciousness • consciousness ranges from stupor to coma • unresponsive to pain, visual, and verbal stimuli • convulsions frequently observed • onset can be gradual or sudden
Complications Associated with Falciparum Malaria • cerebral malaria • anemia • hyperpyrexia • hypoglycemia • acidosis • GI and liver syndromes • pulmonary edema • blackwater fever • algid malaria (shock)
Features Indicating Poor Prognosis in Severe Malaria • impaired consciousness • repeated convulsions • respiratory distress • shock • acidosis/hyperlactemia • hypoglycemia • jaundice or other liver malfunctions • renal impairment • high parasitemia (>500,000/mm3)
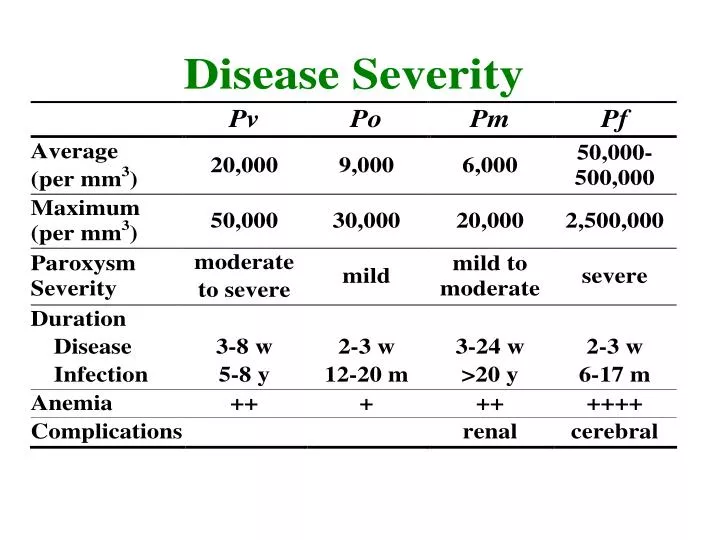
Higher Parasitemias in Falciparum Malaria • all erythrocytes invaded • Pv/Po = reticulocytes • Pm = senescent RBC • up to 36 merozoites • sequestration of infected erythrocytes • trophozoite and schizont stages • primarily in brain, heart, lungs, and gut • complications • immune evasion
avoidance of spleen • low oxygen tensions • better invasion
P. falciparum expresses ‘knobs’ on the surface of infected erythrocytes. Knobs mediate cytoadherence to endothelial cells.
Several Parasite Proteins Are Associated with Knobs • KAHRP and PfEMP2 are believed to interact with the submembrane cytoskeleton of the host erythrocyte • reorganization of the membrane skeleton may result in knob formation • PfEMP1 crosses the erythrocyte membrane and is exposed on the surface
PfEMP-1 Structure • family of 40-50 var genes • conserved intracellular C-terminus • acidic terminal segment (ATS) • binds cytoskeleton + KAHRP • transmembrane domain • variable extracellular domain composed of modules • 2-7 copies of Duffy-binding like domains • 5 sequence types (a, b, g, d, e) • 1-2 cys-rich interdomain regions • all have DBL1a + CIDR • participates in cytoadherence
Possible Host Receptors • CD36 • Ig super-family • ICAM-1 • VCAM-1 • PECAM-1 • E-selectin • thrombospondin • chondroitin sulfate A • hyaluronic acid • Rosetting Receptors • CR-1 • glycosaminoglycan • blood group A
Sequestration Hypothesis cytoadherence cerebral ischemia hypoxia, metabolic effects coma death
Problems with Sequestration Hypothesis • rapid reversibility • lack of ischemic damage • low levels of permanent neurological damage • sequestration occurs in non-cerebral malaria cases
Cytokine Theory Problem • minimal lymphocyte infil-tration or inflammation
Severe falciparum malaria • potentially high parasitemias • sequestration • complex (and not fully understood) host-parasite interactions