Download
1 / 83
920 likes | 1.36k Views
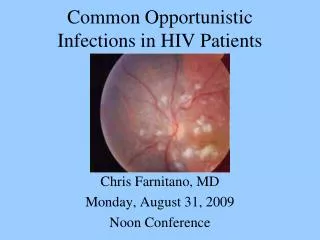
HIV-Associated Opportunistic Infections 2009. Robert D. Harrington, M.D. University of Washington. MMWR 1981. CD4 Count and Opportunistic Infections. CD4 Cell Count. Bacterial Pneumonia, TB, HSV, Cryptosporidiosis. 1,000. Thrush, lymphoma, KS. 500. 200. PCP. 100.

E N D
HIV-Associated Opportunistic Infections 2009 Robert D. Harrington, M.D. University of Washington
CD4 Count and Opportunistic Infections CD4 Cell Count Bacterial Pneumonia, TB, HSV, Cryptosporidiosis 1,000 Thrush, lymphoma, KS 500 200 PCP 100 MAC, CMV, PML, PCNSL, Cryptococcus, Microsporidia Toxo 4-8 Weeks Up to 12 Years 2-3 Years
Common OIs PCP MAC Candida Regional Effects Southwest: Coccidiodomycosis Midwest: Histoplasmosis and Blastomycosis South: Blastomycosis and Toxoplasmosis Opportunistic Infections and Geography North America
Opportunistic Infections and Geography PCP, TB Candida, MAC Cryptococcus Leishmaniasis The World PCP TB Candida Cryptococcus Penicilliosis Candida PCP MAC TB Bacteria Malaria Cryptococcus PCP TB Cryptococcus Isospora Cryptosporidiosis Microsporidia Holmes, CID, 03 Putong, SEA Trop Med, 02 Margues, Med Mycol, 2000 Amornkul, CID, 03
Prophylaxis to Prevent Opportunistic Infections Considerations for Prophylaxis • Infection should be common and/or predictable • Infection should be clinically significant • Treatment (prophylaxis) should be effective, non-toxic and affordable
Primary PCP CD4 < 200 MTb PPD > 5mm Toxo IgG+,CD4 < 100 MAC CD4 < 50 VZV Exposure with IgG- or no hstry S. pneumoniae HBV HAV Influenza Secondary PCP Toxo MAC CMV Cryptococcosis Histoplasmosis Coccidioidomycosis Salmonella species bacteremia Recurrent HSV Recurrent Candidiasis Prophylaxis to Prevent Opportunistic Infections in the Developed World
Effect of HAART on Opportunistic Infections: Reduced Need for Prophylaxis Primary Prophylaxis PCP When CD4 > 200 for 3 months MAC When CD4 > 100 for 3 months Toxo When CD4 > 200 for 3 months
Effect of HAART on Opportunistic Infections: Reduced Need for Prophylaxis Secondary Prophylaxis or Maintenance Therapy PCP When CD4 > 200 for 3 months CMV When CD4 > 100-150 for 6 months, retinal disease stable and not sight- threatening MAC When CD4 > 100 for 6 months, no symptoms of MAC and after 12 months of MAC Rx Toxo When CD4 > 200 for 6 months and completed initial Toxo Rx Cryptococcus When CD4 > 100-200 for 6 months and completed initial Crypto Rx
HIV ASSOCIATED MALIGNANCIES AIDS Defining Malignancies • Kaposi’s sarcoma • Primary CNS lymphoma (PCNSL) • Non-Hodgkin’s lymphoma (NHL) • Invasive cervical cancer
Hodgkin’s disease Anal cancer Multiple myeloma Leukemia Lung cancer Head and neck tumors GI malignancies Genital cancers Hypernephroma Soft tissue tumors HIV ASSOCIATED MALIGNANCIES Increased Rates of Other Cancers in HIV
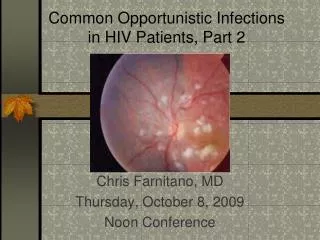
Case 1 • A 42 year old man with HIV (CD4 89) presents with fever, headache, fatigue and recurrent molluscum contagiosum. • Blood cultures are taken, his molluscum lesions are treated with liquid nitrogen, he is given Tylenol for his fevers and goes home. • He returns several days later more lethargic with a worsening headache, a temperature of 39 degrees C and more molluscum lesions.
Case 1 What questions do you have regarding his history and physical exam? • Does he have any pulmonary symptoms? • What is his TB exposure and testing history? • Where has he lived? • What animal and environmental exposures does he have? • What is his toxoplasmosis serology? • Has he had other infections in the past? • Tell me more about these skin lesions. Can I see them?
Case 1 Mandell, Atlas of Infectious Diseases
Case 1 What diagnostic testing do you want? • Brain CT is negative • CSF analysis: opening pressure is 300 mm, WBC 0, protein 60, glucose 30, CRAG is negative, VDRL is negative, PCR for CMV, VZV, HSV and EBV are negative
Case 1 Does he have meningitis? What is your differential diagnosis? • Cryptococcal meningitis • Bacterial meningitis (S. pneumoniae, H. influenza, N. meningitidis, L. monocytogenes) • Tuberculous meningitis • Other chronic meningitides (histoplamosis, blastomycosis, etc) • Viral meningo-encephalitis (e.g., HSV, enteroviruses, other herpes viruses, rabies
Case 1 What test do you want next? Mandell, Atlas of Infectious Diseases
Case 1 Silver stain of CSF capsule Narrow base Mandell, Atlas of Infectious Diseases
Case 1 Why was the CSF CRAG negative? Antigen excess (the prozone phenomenon)
Case 1 How are you going to treat him? • Initial therapy; AmphoB (0.7 mg/kg/d) with or without 5-FC for 2 weeks • Followed by fluconazole at 400 mg/day for 10 weeks and then maintenance therapy with fluconazole at 200 mg/day. • Relapse without suppressive therapy (or HAART) is 50 to 60% (Van der Horst, NEJM, 1997) (Saag, CID, 2000)
Case 1 • High pressure associated with more symptoms (HA, meningismus, cranial nerve deficits) and higher antigen titers. • Pressure > 350 is associated with early (first week) death • Most experts recommend serial large volume spinal taps or spinal drains for patients with elevated CSF pressures Anything else? (Graybill, CID, 2000)
Case 1 How will you follow him? • Cryptococcal antigen for monitoring therapy: • Serum; No: no correlation between titer and outcome • CSF; Yes: unchanged or rising titer is associated with failure and relapse. • High dose steroids associated with increased mortality (Powderly, CID, 1994)
Case 1 When should you provide HAART?
Timing of HAART #142: Immediate Vs Delayed ART in Setting of Acute OI, Zolopa, Powderly, et.al. (ACTG 5164) • Randomized study of ARV given within 14 days of Rx for OI Vs delayed (at least 4 wks) • Patients with TB excluded • Primary endpoint: 48 week combination of 3 categorical variables • 1. Death or alive with new AIDS diagnosis • 2. Alive with HIV RNA > 50 and no new AIDS diagnosis • 3. Alive with HIV RNA < 50 and no new AIDS diagnosis
Timing of HAART #142: Immediate Vs Delayed ART in Setting of Acute OI, Zolopa, Powderly, et.al. (ACTG 5164) • Patients (N=282) • Median age 38 • Median CD4 = 29 and log10 HIV RNA level = 5.07 • OIs • PCP 63% • Cryptococcal meningitis 13% • Pneumonia 10% • Median time to starting ART 12 Vs 45 days
Timing of HAART ACTG 5164: Results • No significant difference between immediate Vs delayed for the composite endpoint • Immediate arm had fewer deaths/new AIDS diagnosis • Immediate arm had longer time to death/new AIDS diagnosis (HR 0.53) P=0.035
Early Vs Delayed HAART in Patients with Cryptococcal Meningitis in Africa(Macadzange,CROI,2009,Abs 38cLB) • Open Label RCT • Patients: Adults with HIV and Cryto meningitis (CSF CrAg or India ink positive) • All received Fluconazole 800 mg PO once daily x 10 wks + aggressive pressure management • Followed by maintenance fluconazole 200 mg • Intervention: d4T, 3TC, NVP • EARLY: Immediate start with initial fluconazole • DELAYED: Start after initial 10 wks of fluconazole • Primary Outcome: Mortality after 2 years
Early Vs Delayed HAART in Patients with Cryptococcal Meningitis in Africa(Macadzange,CROI,2009,Abs 38cLB) TOTAL: 50 patients Overall 2-yr Mortality: 62% DELAYED 23 patients Median Survival: 274 days 2-yr Mortality: 37% EARLY 27 patients Median Survival: 35 days* 2-yr Mortality: 87%** *Comparison of median survival, p=0.03 **Comparison of 2-yr Mortality, p=0.002
Early Vs Delayed HAART in Patients with Cryptococcal Meningitis in Africa(Macadzange,CROI,2009,Abs 38cLB) All but 2 deaths due to Cryptococcus Other 2 deaths ascribed to TB-IRIS Baseline CD4 cells similar in those who died in each group
Case 2 • A 38 yo South African male presents with a 10 kg weight loss, 10 weeks of cough and intermittent fever. He has no past medical history. • On exam he is thin, T 38.8 C, BP 100/70, HR 104, RR 20. He has prominent cervical adenopathy, oral thrush and course breath sounds over his R upper and mid lung zones.
Case 2 Initial CXR for Case 2 • What diagnostic tests do you want? • “HIV test is + and Sputum smear stains 3+ for AFB”
Case 2 • He is admitted to a hospital ward with similar patients and started on “RIPE” therapy. • After a week his constitutional symptoms improve. His CD4 T-cell count measures 15 cells/uL. • Should he be offered HAART? • If so, when should HAART be started? • Are there TB and HIV drug interactions of concern?
Immune Reconstitution Syndrome TB-IRS and CD4 and HAART • TB-associated IRS in South Africa • 160 patients receiving Rx for TB at the time HAART initiated • Median CD4 68 • IRS in 12% overall, 32% in those who started HAART within 2 months of TB Rx • MV analysis: IRS risks • Low CD4 • Early HAART – OR for starting HAART < 30 days = 69.5 • 2 IRS deaths (both had disseminated TB (Lawn, AIDS 2007;21:335-41)
SAPiT(Karim,CROI,2009,Abs36a) • Open-label RCT • Patients • Smear positive and on standard TB tx regimen • HIV positive with CD4 cell count < 500 • ART: ddI + 3TC + EFV once daily with TB DOT • Endpoints • Primary: all cause mortality • Secondary: Tolerability, toxicity, viral load, CD4 count, TB outcomes and IRIS
SAPiT(Karim,CROI,2009,Abs36a) Study Arms • Integrated TB-HIV treatment 1. ART initiated as soon as possible during the intensive phase of TB tx (first 8 weeks) 2. ART initiated after the intensive phase of TB tx • Sequential – ART initiated after TB tx completed
WHO/DHHS: Treatment HIV-TB Pulmonary TB Extrapulmonary TB CD4 < 100 Start TB therapy, start HAART in 2 weeks Start TB therapy HAART as soon as TB Rx tolerated (b/n 2-8 wks) Some experts would wait until 8 weeks (avoid IRIS) CD4 100-200 Start TB therapy HAART after intensive phase of TB Rx (HAART earlier if severely immunocompromised) CD4 200-350 Start TB therapy Monitor CD4 count and start HAART when indicated CD4 > 350 CD4 not available TB therapy Improving, no OIs HAART when TB Rx complete
TB/HIV Co-infection: Principles of Treatment • Treatment generally the same as in HIV- patients (4 drugs for 2 months and 2 drugs for 4 months) • Sub-optimal response (culture + after 2 months) – give 9 months, skeletal TB – 6 to 9 months, CNS TB – 9 to 12 months • If using regimens without INH or a rifamycin - duration should be 12 to 15 months
Principles of Treatment:Importance of Rifamycin • Treatment with NON rifamycin-containing regimens is associated with: • Higher relapse rates • Higher mortality Wallis, et al. (1996) Tuber Lung Dis 77:516-23 Hawken, et al. (1993) Lancet 342:332-38 Perriens, et al. (1991) AM Rev Resp Dis 144:750-55 Korwnromp, et al. (2003) CID 37:101-12
Principles of Treatment • Be wary of drug interactions between the rifamycins and HIV medications • Do not use TB treatment regimens that are dosed weekly (e.g. INH-rifapentine) or even twice weekly in patients with CD4 counts < 100 • Consider measuring drugs levels if there is concern for malabsorption or increased elimination of TB therapies
Principles of Treatment Drug Interactions: The P450 system • Isoform CYP 3A is affected and/or involved in the metabolism of rifamycins, NNRTI and PIs • Rifamycins: Induce CYP 3A • Rifampin > rifapentine > rifabutin • Rifampin is not metabolized by CYP 3A (level not affected by other drugs that influence CYP 3A) • Rifabutin is metabolized by CYP 3A (level is affected by other drugs that also affect CYP 3A)
Principles of Treatment • If using rifampin - avoid PI-based HAART - use NNRTIs (EFV preferred over NVP) • If using rifabutin - can use PIs or NNRTI - but will have to dose adjust the rifabutin in most cases
Principles of Treatment Web site for more complete table showing dosages: http://www.cdc.gov/tb/TB_HIV_Drugs/Table1.htm Also tables 2 and 3
Case 2 …back to the case • 10 days into his TB therapy he is started on HAART. • 3 weeks later his fever and cough return
Case 2 Follow up CXR for Case 2 • What are you worried about and what are you going to do?
XDR TB # 143: Exogenous Re-infection with MDR and XDR TB Among TB/HIV Infected Patients in Rural South Africa, Andrews, et.al. • Case control study of patient with pulmonary TB at Church of Scotland Hospital, South Africa from 2005-06 • N=170; 43 had baseline and follow-up cultures; 23 developed MDR or XDR TB
XDR TB # 143: Exogenous Re-infection with MDR and XDR TB Among TB/HIV Infected Patients in Rural South Africa, Andrews, et.al. 170 patients with TB 43 had both initial and follow up cultures done 23 developed MDR or XDR TB 17 had paired spoligotypes performed 17/17 pairs were NOT matched