Bowel Elimination
230 likes | 684 Views
Bowel Elimination. Dr. Belal Hijji, RN, PhD March 10 & 17, 2012. Learning Outcomes. After this lecture, students will be able to: Describe the anatomy and physiology of the GIT Identify common bowel elimination problems and factors influencing elimination

Bowel Elimination
E N D
Presentation Transcript
Bowel Elimination Dr. Belal Hijji, RN, PhD March 10 & 17, 2012
Learning Outcomes After this lecture, students will be able to: • Describe the anatomy and physiology of the GIT • Identify common bowel elimination problems and factors influencing elimination • Describe factors affecting bowel elimination • Discuss nursing assessment and diagnostic tests. • Discuss nursing interventions for selected alterations in bowel function.
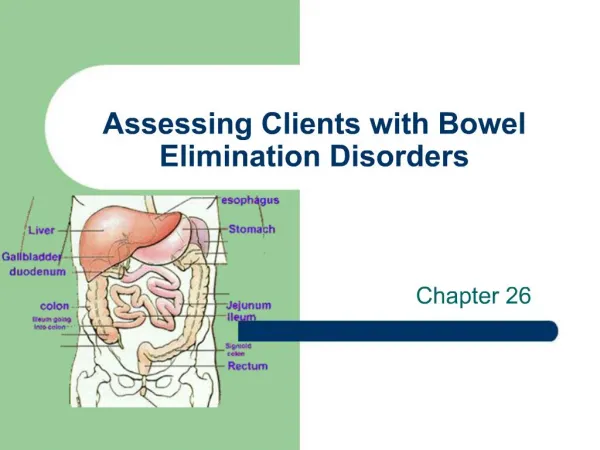
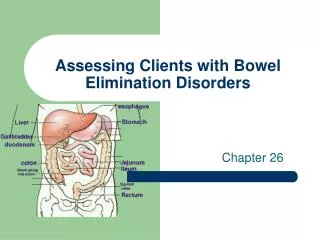
Anatomy and Physiology of the GIT • Mouth: The mouth mechanically and chemically breaks down nutrients into usable size and form. Digestion begins in the mouth and ends in the small intestine. • Oesophagus: As food enters the upper esophagus, it passes through the upper oesophageal sphincter. This sphincter is a circular muscle that prevents air from entering the esophagus and food from refluxing into the throat. • Stomach: Has three functions: the storage of swallowed food and liquid; mixing of food, liquid, and digestive juices; and emptying its contents into the small intestine. The stomach produces and secretes hydrochloric acid (HCL), mucus [protective], pepsin, and intrinsic factor [for absorption of vitamin B12).
Small intestine: Is divided into the duodenum [2 feet], the jejunum [9 feet], and the ileum [12 feet]. Most nutrients and electrolytes are absorbed in the small intestine. • Large intestine (lower GIT): Is divided into the cecum, colon, and rectum. The colon has three tasks: absorption, secretion, and elimination.
Anus: Is the place where feces is expelled out of the body. The anal canal is richly supplied with sensory nerves that help to control continence. • Defecation: The physiological factors critical to bowel function and defecation include normal GIT function, sensory awareness of rectal distension and rectal contents, voluntary sphincter control, and adequate rectal capacity and compliance
Common Bowel Elimination Problems • Constipation: Constipation is the infrequent and difficult passage of hardened stool. Constipation can be caused by certain medications (ie, antidepressants, antihypertensives, opioids, antacids with aluminum, and iron); rectal or anal disorders (eg, hemorrhoids, fissures); obstruction (eg, cancer of the bowel); metabolic and neuromuscular conditions (eg, diabetes mellitus, multiple sclerosis); and endocrine disorders (eg, hypothyroidism, pheochromocytoma). Other causes include weakness, immobility, and an inability to increase intra-abdominal pressure to facilitate the passage of stools. Constipation results from dietary habits (ie, low consumption of fiber and inadequate fluid intake), lack of regular exercise, and a stress-filled life. • Impaction: Results from unrelieved constipation, whereby hardened faeces cannot be expelled for several days despite repeated urge to defecate. Impaction develops in patients who are unconscious, badly constipated, or those with interrupted nerve supply to bowel.
Diarrhea: Is an increased frequency in the passage of loose stools which may lead to fluid and electrolyte imbalance. Causes of diarrhea include infectious agents (Clostridium difficile, Escherichia coli, Salmonella, Shigella, Entamoeba histolytica, and Giardia), inflammatory bowel disease, short bowel syndrome (due to reduced surface area for reabsorption), side effects of drugs (multiple antimicrobial agents can promoting an overgrowth of C. difficile in the bowel; and laxative or enema misuse).Intestinal contents are irritating and can lead to skin breakdown in the perianal region. The aim of treating diarrhea is to maintain adequate hydration and electrolyte balance.
Incontinence: Fecal incontinence is the involuntary loss of stool of sufficient magnitude to create a social or hygienic problem. When impaction of stool develops, bacteria in the rectum overgrow, producing a liquefied stool. The toxins produced by this medium can stimulate the bowel and may produce transient seepage of stool in the normally continent client. Sensory disorders interferes with the client’s ability to differentiate gas and solid and liquid contents in the rectum. Anatomic disorders also may compromise sphincter function. Women are at risk for obstetric trauma. Vaginal deliveries, requiring the use of forceps, are likely to damage the anal sphincter mechanism.
Factors Influencing Bowel Elimination • Age: Ability to control defecation occurs at the age of 2-3 years. In older adults, peristalsis declines, esophageal emptying slows. Muscle tone in the perianal floor and anal sphincter weakens, causing difficulty in controlling defecation. • Diet: Regular daily food intake, high-fiber foods, raw or cooked fruits, vegetables, and cereals and bread promote peristalsis. Low-fiber foods (lean meats, milk) slow peristalsis. Gas producing foods (broccoli, cauliflower, onions, dried beans) can stimulate peristalsis. • Position during defecation: Squatting allows a person to lean forward, exert intraabdominal pressure, and contract thigh muscles to normally defecate. Immobilised client using a bedpan cannot contract muscles to defecate.
Pregnancy: Pressure adds to the rectum leading to constipation. • Diagnostic tests: Examination of the GIT structures require emptying of bowel contents. NPO status, bowel evacuants, and cleansing enemas are factors that interfere with normal elimination. • Fluid intake: Water liquefies intestinal contents for easier passage. Hot beverages and fruit juices soften stool and increase peristalsis. Large quantities of milk may slow peristalsis and cause constipation. • Activity: immobilisation depresses colon motility and regular physical exercise promotes peristalsis. • Psychological factors: Anxiety or fear can accelerate digestion and peristalsis. Diarrhea may result. • Pain: Can suppress defecation resulting in constipation.
Assessment • Health history: Because issues of elimination may produce feelings of anxiety, guilt, or shame among clients, the interview must be instigated by the nurse and conducted in a setting that provides adequate privacy. The nurse should ask clients to describe their usual elimination habits, the nature of the current problem and its duration, the types of food that cause diarrhea, and identify the bowel management programme such as how bowel is evacuated, regular use of laxatives, suppositories, or enemas). • Physical exam: Mental status can be evaluated by listening to the client’s responses to questions and by observing interactions with others. Continued…
Physical exam (continued…): The nurses should assess mobility and dexterity. Mobility may be evaluated by observing the client undress or move onto a table, chair, or bed. Dexterity [skill] is assessed by observing the client remove clothing; particular attention is paid to the manipulation of zippers, buttons, and shoestrings. The perineum is initially inspected for skin integrity. Among patients with severe fecal incontinence, the skin is frequently red and painful to touch, due to exposure to liquid stool. The integrity of the skin typically remains intact with mild to moderate fecal incontinence.
Diagnostic and Laboratory Data • A stool culture for ova and parasites, electrolytes, or when gastrointestinal infection is thought to be causing diarrhea and related incontinence.
Planning • Maintain elimination health • Initiate exercise regimen • Initiate diet and fluid therapy • Administer medications • Administer enema
Maintaining Elimination Health • Fluid intake: Clients should be taught to drink an adequate amount of fluid each day, which is 30 ml/kg body weight. In the average-sized adult, this equals 1500 to 2000 ml/d. • Diet: Dietary fiber may prevent constipation and increase the desire to defecate. The client is taught to increase gradually the amount of fiber-rich foods in the diet, including grains, fruits, and vegetables. • Lifestyle and prevention: Smoking stimulates the bowel causing increased bowel tone and motility, resulting in diarrhea. Acute and chronic stress affect bowel by increasing its activity. Managing stress promotes healthy bowel elimination patterns. Nurses are in position to educate clients on how to manage stress (This will be discussed later).
Elimination habits: The client is urged to establish a regular schedule of bowel elimination and to answer the desire to defecate, as routine avoidance may predispose to constipation and reduce the efficiency of bowel evacuation. The urge to defecate is typically greatest after a meal, and it may be enhanced by dietary stimulants such as fiber or a caffeinated beverage or by light exercise. • Positioning: Positioning of the client plays an important role in elimination. Sitting is the usual position for a client for bowel elimination. Clients unable to use the toilet require assistance in accomplishing elimination. Devices such as the bedpan or commode can be used
Initiate Exercise Regimen • Regular exercise leads to good muscle tone and stimulates the bowels to move regularly. • Inadequate tone in the abdominal muscles, diaphragm, and the perineal muscles can cause difficult defecation. If a client is suffering from constipation, a regimen of walking or light recreational exercise should be recommended to promote peristalsis and defecation.
Initiating Diet and Fluid Therapy • Dietary fiber and fluid intake can be increased to promote the passage of soft, hydrated stool. The client who is unable or unwilling to obtain adequate fiber from the diet may be given a bulk laxative (such as Metamucil) or a bran mixture as a specific dietary supplement. Initially, 3 to 6 grams of the supplement is administered, and the dosage is gradually increased until a soft, well-formed stool is obtained. • The initial management of diarrhea involves the removal of factors that predispose the individual to the condition and the maintenance of adequate fluid and electrolyte balance. Persons with infectious diarrhea are given antimicrobials to destroy the pathogens that produce diarrhea.
Administering Medications • Constipation is initially managed by assisting the individual to pass hardened stool or by removing any impacted feces. Bowel evacuation is encouraged by an oral laxative, such as psyllium. • Constipation resulting in an impaction requires mechanical disruption and removal, followed by a cleansing enema or an oral laxative. Alternatively, a pulsed irrigation enhanced evacuation (PIEE) system can be used. The PIEE uses gravity to deliver intermittent pulses of warmed saline to break up and remove hardened and impacting fecal material.
Administering Enema • Enema administration is a procedure used to introduce fluid into the lower bowel. The purpose of an enema is to cleanse the lower bowel, to assist in the evacuation of stool or flatus, or to instill medication. See next slide for the types of enemas, along with the solutions and the indications for use of each. • Enemas can be large (500 to 1000 ml) or small (150 to 240 ml) depending on their purpose. Large-volume enemas are administered to cleanse the bowel. Small-volume enemas are used for the purpose of evacuating stool or instilling medications in the lower bowel. Caution should be used when administering large volume enemas, because fluid and electrolyte imbalance can occur.