Download
1 / 25
270 likes | 584 Views
TREATMENT OF ACUTE CORONARY SYNDROMES. At the end of this self study the participant will: Describe ACS risk stratification List goals of medication therapies Describe complications of ACS. Treatment depends on the patient’s identified risk. Low risk Intermediate risk High risk.

E N D
TREATMENT OF ACUTE CORONARY SYNDROMES At the end of this self study the participant will: • Describe ACS risk stratification • List goals of medication therapies • Describe complications of ACS.
Treatment depends on the patient’s identified risk • Low risk • Intermediate risk • High risk
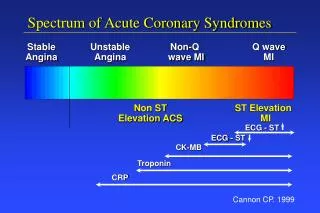
ACS Risk Stratification Taken from http://www.aafp.org/afp/20050701/119.html
Low Risk Medical Management • ASA • NTG (PO/NTP) • Consider • BetaBlocker • Stress Test • Risk factor modification • Statin • Discharge/Admit to Chest Pain Center
Intermediate Risk Medical Management • Oxygen (if O2 sat < 90%) • ASA, Clopidogrel if ASA intolerant/ sensitive • NTG (PO/NTP/Spray) • LMWH/ Unfractionated Heparin • -Blocker • ACE inhibitor: EF < 40% • Statin • Consider Echocardiagram, stress test • Admit to Telemetry Braunwald, et al, http://www.acc.org/clinical/guidelines/unstable/unstable.pdf accessed April 2, 2002.
Medical Management High Risk UA/Non-STEMI • Oxygen (if O2 sat < 90%) • ASA, Clopidogrel if ASA intolerant/ sensitive • Clopidogrel if medical management/ PCI • Enoxaparin • NTG (IV/PO/NTP) • -Blocker • ACE inhibitor: ejection fraction <40% • Statins • Consider Echocardiogram • Admit to CCU/Telemetry Braunwald, et al, http://www.acc.org/clinical/guidelines/unstable/unstable.pdf accessed April 2, 2002.
Aggressive Management High RiskUA/Non-STEMI (Cath, PCI, CABG) • Oxygen (O2 sat < 90%) • Clopidogrel if ASA intolerant/ sensitive • Clopidogrel in addition to ASA • LMWH or Unfractionated Heparin • NTG (IV/PO/NTP) • -Blocker • GP IIb-IIIa Inhibitor for PCI • Cardiac Catheterization Braunwald, et al, http://www.acc.org/clinical/guidelines/unstable/unstable.pdf accessed April 2, 2002.
Medical ManagementAcute STEMI • Oxygen (O2 sat < 90%) • NTG SL • ASA • Unfractionated Heparin • IV Nitroglycerin • IV Morphine Sulfate • Fibrinolytic Therapy (if candidate) or Primary PCI • Consider Beta Blocker; Consider ACE-I • Admit to CCU or Arrange for PCI *Ryan et al, JACC 1999;34(3):890-911.
Thrombolytic or Fibrinolytic Agents (start within 30 minutes of “door”) Goal: break down clots allowing perfusion (remember destroys all clots, not just those in coronary arteries) Reteplase (rPA) • treatment of MI; double bolus Tenecteplase (TNK) • treatment of MI; single bolus Alteplase (tPA) • treatment of ischemic stroke, PE, catheter declotting; bolus followed by an infusion Combination Therapy: Fibrinolytic, plus IIb/IIIa inhibitor
Antiplatelet Agents • Goal: Prevent further clotting by preventing platelet aggregation • Salicylates: All ACS • ASA (chewed for acute chest pain) • ADP-receptor inhibitors: UA, stents • Clopidigrel (Plavix) • Glycoprotein (GP) IIb-IIIa receptor antagonists: Non-STEMI, UA • Abciximab (ReoPro) • Eptifibatide (intergrelin) • Tirofiban (Aggrastat)
Antithrombin Agents • Goal: Prevent further clotting by thrombin inhibition, either directly or indirectly • Heparin -unfractionated heparin (UFH) • Low–molecular-weight heparins (LMWH) with UA/NSTEMI indications (not indicated for STEMI) • enoxaparin • dalteparin • Direct-acting antithrombins • Bivalirudin (angiomax) • argatrobran • lepirudin Incredible Machine. National Geographic Society. 1986. Used by Permission
Vitamin K Antagonists • Goal: Prevent clotting through oral therapy • Coumadin (Warfarin) • Chronic Atrial Fibrillation • Prosthetic Valves • Mural Thrombus
Actions: myocardial 02 demand, heart rate, arrhythmias Contraindications: avoid in bronchospastic diseases, cardiac failure, severe abnormalities in cardiac conduction, hypotension and insulin dependent diabetics Adjunctive Therapy: Beta Blockers-lol drugs
Actions: decrease afterload, reduce compensatory LV hypertrophy, improve ejection fraction, limit size of infarct Contraindications: hypotension, renal artery stenosis, allergy to ACEs Adjunctive Therapy: ACE Inhibitors-pril drugs
Actions: dilates coronary arteries, increases collateral blood flow, decreases preload & afterload Contraindications: hypotension, marked bradycardia, hypersensitivity to nitrates Adjunctive Therapy: IntravenousNitroglycerin
Lipid Lowering Agents • Lower LDL and increase HDL when combined with Statin • Niacin, Lopid, Questran, etc.
STATINS • Lowers Low Density Lipoproteins (LDL) • May help to decrease accumulation of plaque • Stabilizes plaque • Reduces chance of plaque rupture • When combined with Niacin, may increase High Density Lipoprotein (HDL). • Lipitor, Pravachol, Zocor, etc.
Coronary Artery Bypass Graft (CABG) • Goal: Surgically enhance circulation • Can use internal mammary artery, radial artery or sapphenous vein • one end is either sewn to the aorta or may remain connected to the larger artery where it originated. • The other end is attached (grafted) beyond the blockage in the coronary artery. • As a result, blood can flow around the blocked area, increasing the supply of oxygen and nutrients to the heart muscle.
Post ACS Complications Left Ventricular Failure • Problem with forward flow (low cardiac output, ejection fraction drops) • Blood backs up into lungs (respiratory implications) Cardiogenic Shock • Severe LV failure • Need to intervene early
Post ACS Complications Ventricular Septal Defect • Hole develops in septum causing oxygenated blood to remix with deoxygenated blood in heart • Problem with forward flow • New systolic murmur, decreased pO2, LV failure Myocardial Rupture • Hole develops in free wall (outside wall) • Problem with forward flow • LV failure, cardiac arrest
Post ACS Complications Papillary Muscle Rupture • AV valve (tricuspid or mitral) leaflets float upward into atria during closure • Blood leaks back into atria during ventricular contraction • Loud new systolic murmur, pulmonary edema, cardiogenic shock
Post ACS Complications Ventricular Aneurysm and Thrombosis • Tend to develop with anterior MI • Risk of mural thrombus causing a PE • High risk for stroke if aneurysm in LV • Dx with ECHO • Anticoagulate
Post ACS Complications Recurrent Ischemia or Infarction • High risk for first 10 days • Especially with non-transmural MI or non Q wave MI • Educate patient about significance of symptoms Pericarditis • Inflammatory reaction of pericardium • Pain with inspiration, splinting, pericardial rub • Referred to as Dressler’s syndrome if 2 weeks to 3 months post MI
References • 1Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE III, Steward DE, & Theroux P. ACC/AHA guidelines for the management of patients with unstable angina and non-ST segment elevation myocardial infarction: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiology 2000;36:970-1062. • 2 The Joint European Society of Cardiology/ American College of Cardiology Committee. Myocardial Infarction Redefined--A Consensus Document of The Joint European Society of Cardiology / American College of Cardiology Committee for the Redefinition of Myocardial Infarction. J Am Coll Cardiol 2000;36:959-969.